This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
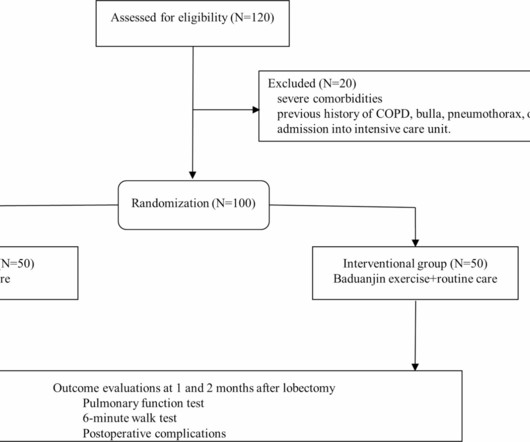
Some pulmonary tuberculosis patients may require lung resection surgery. Postoperative pulmonary rehabilitation is essential to restore the lung function and maintain quality of life. We aimed to study the pul.
For a 10-minute video review on reading Pulmonary CT Scan — WATCH_this_VIDEO by Dr. Jake Gibbons. Figure-5: CTPA view in today's case — showing large clot burden in the right and left main pulmonary arteries. == C ASE F ollow-Up: The "good news" in today's case — is that the patient received thrombolytics, and ultimately did well.
However, at the time, we did not know he also had a very rare isolated left pulmonary artery (causing PPHN) as this was hard to detect on the ultrasound and would later be detected at his cath. When the day came that it was time to say goodbye to Austin, the doctors and nurses were right next to us every step of the way.
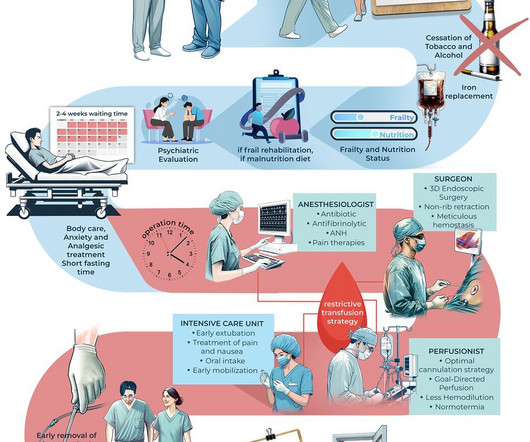
4) Rehabilitation; Physical and pulmonary rehabilitation. (5) By the addition of well-established and nurse-based ERAS protocols, complication and transfusion rates can be decreased, early recovery and discharge can be provided. 2) Anemia; diagnostic evaluation and its treatment by iv iron. (3) 5) Anxiety and Analgesia treatment. (6)
In addition to being led by the American Heart Association and the American College of Cardiology Joint Committee on Clinical Practice Guidelines, the guideline was developed with and endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Podiatric Medical Association, the Association of Black Cardiologists, (..)
This educational event covers coding specific to cardiothoracic surgery, with concentrations in Evaluation and Management (E/M) visits, Adult Cardiac Surgery, Congenital Heart Surgery, General Thoracic Surgery (Esophagus, Mediastinum, Pulmonary), and Vascular Surgery.
This educational event covers coding specific to cardiothoracic surgery, with concentrations in Evaluation and Management (E/M) visits, Adult Cardiac Surgery, Congenital Heart Surgery, General Thoracic Surgery (Esophagus, Mediastinum, Pulmonary), and Vascular Surgery.
Twenty-four experienced practitioners (including physicians, nurses, pharmacists, and a respiratory therapist) from multiple medical specialties, levels, institutions, and countries made up the panel. Topics were identified and prioritized by the panel and arranged by organ system to facilitate discussion, debate, and consensus building.
The Challenges Ascension Saint Thomas Hospital, based in Nashville, Tennessee, encountered persistent issues with missing documentation, including anesthesia records, Intraoperative Transesophageal Echocardiograms, perfusion records, and Pulmonary Function Test results.
Gender disparities were also observed, with more self-pay males discharged to skilled nursing facilities compared to females (3.8% Patients were drawn from neurology, cardiology, and other services. Discharge disposition varied by age and insurance status; insured elderly patients were more likely to be discharged to extended care facilities.
This educational event covers coding changes specific to cardiothoracic surgery, with concentrations in Evaluation and Management (E/M) visits, Adult Cardiac Surgery, Congenital Heart Surgery, General Thoracic Surgery (Esophagus, Mediastinum, Pulmonary), and Vascular Surgery. Post-pandemic changes to telehealth will be discussed.
The Challenges Ascension Saint Thomas Health, based in Nashville, Tennessee, encountered persistent issues with missing documentation, including anesthesia records, Intraoperative Transesophageal Echocardiograms (TEE), perfusion records, and Pulmonary Function Test (PFT) results.
However, the triage nurse wrote a note saying that he did admit to chest pain yesterday, which he vaguely endorsed when questioned again. The D-dimer was elevated at 942, and the subsequent CT angiogram of the chest showed bilateral lower lobe subsegmental pulmonary emboli with a small right pleural effusion.
One of my most talented readers is a health care assistant (a nursing assistant) who has taken a keen interest in ECGs. Was there pulmonary edema? My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. And they teach me a lot. He can beat nearly anyone.
hours total) Joseph Turek, MD, Jeffrey P. hours) Session 7: (1.75 Upon completion of this activity, participants should be able to: Identify new CPT codes, updates, and payment policies affecting cardiothoracic surgery coding for 2023.
CT angiogram chest: no aortic dissection or pulmonary embolism. Serial chest xrays: progressive bilateral pulmonary edema. He spent several days in the PICU, undergoing workup including: Serial troponins: rising from 5,700 ng/L (unknown if I or T) to greater than 25,000 ng/L (greater than the lab's upper limit of reporting).
In the evening, a middle-aged man complained of chest pain at the nursing home. Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. He was awake, with a pulse of 130 and BP of 50/30. Fluids were started. The patient arrived alert but cool and clammy. His chest pain was vague. He complained of chronic dyspnea.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. It would be difficult to get a nurse to give it faster! Medics stated that he had not been taking his clopidogrel for 2 weeks. He appeared to be in shock. Here is his ED ECG: There is obvious infero-posterior STEMI.
COPD, chronic obstructive pulmonary oedema; HR, hazard ratio; ICU, intensive care unit; LTI, long-term illness; RR, rate ratio; SoC, standard of care. The RMP included a digital interface for proficient patients and phone monitoring by nurses for those uncomfortable with digital technology.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content