This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Image courtesy: Philips christine.book Wed, 06/12/2024 - 14:07 June 12, 2024 — Royal Philips has announced its next-generation AI-enabled cardiovascular ultrasound platform to help speed up cardiac ultrasound analysis with proven AI technology and reduce the burden on echocardiography labs.
Sympathetic overactivation and neuroinflammation in the paraventricular nucleus (PVN) are crucial factors in post-myocardialinfarction (MI) cardiac remodeling and ventricular arrhythmias (VAs). Meanwhile, the cGAS-STING pathway has shown potential to ameliorate neuroinflammatory response.
A new study by researchers at Karolinska Institutet and Sdersjukhuset shows that advanced ultrasound imaging analyses cannot identify patients who would benefit from beta-blocker treatment after a myocardialinfarction.
Our previous study showed that light-emitting diode (LED) modulation of hypothalamic paraventricular nucleus (PVN), which is the control center of the sympathetic nervous system, might attenuate neuroinflammation in PVN and prevent ventricular arrhythmias (VAs) after myocardialinfarction (MI).
The 2 coprimary outcomes were target lesion revascularization and myocardialinfarction. The secondary outcomes included ischemia-driven target lesion revascularization, target vessel myocardialinfarction, death, cardiac death, target vessel revascularization, stent thrombosis, and major adverse cardiac events.
Introduction Intravascular ultrasound (IVUS) improves clinical outcome in patients undergoing percutaneous coronary intervention (PCI) but dedicated prospective studies assessing the safety and efficacy of IVUS guidance during primary PCI are lacking.
Myocardialinfarction with non-obstructive coronary arteries (MINOCA) defines a heterogeneous group of atherosclerotic and non-atherosclerotic conditions, causing myocardial injury in the absence of obstructive coronary artery disease.
An emergency cardiac ultrasound could be very useful. The upright portion of the T-wave in aVF is very large compared to the QRS size. These findings mandate that the patient at least get serial ECGs. If these remain unchanged, then serial troponins.
Bedside cardiac ultrasound with no obvious wall motion abnormalities. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. He was started on nitro gtt.
However, the patient's cardiac Doppler ultrasound indicated poor cardiac contractions, and extracorporeal membrane oxygenation (ECMO) was started immediately. We administered adrenaline for cardiac excitation, dopamine for maintained blood pressure, sodium bicarbonate to correct the acidosis, and multiple electric defibrillations.
But there are also new Q-waves, stronly suggesting new infarction. A bedside cardiac ultrasound performed by a true EM expert (Robert Reardon, who wrote the cardiac ultrasound chapter in Ma and Mateer) showed an inferior wall motion abnormality. Overall interpretation: this does not look like OMI to me.
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
Background:The no-reflow has been reported to be associated with larger infarct size and mortality after acute myocardialinfarction (AMI). The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The
A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. Angiogram: "ACS - Non ST Elevation MyocardialInfarction. This is a HUGE myocardialinfarction. There was no cough or fever, the CXR looks like pulmonary edema, the ultrasound showed classic pulmonary edema B lines.
and European societal guidelines that intravascular imaging with either optical coherence tomography (OCT) or intravascular ultrasound (IVUS) should be routinely used during complex coronary stent procedures, s ays first authorGregg W. These results extend the strong recommendations from recent U.S.
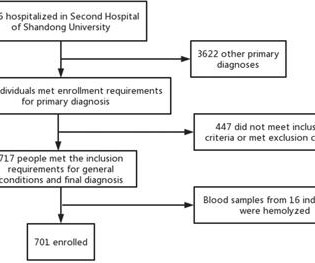
Background To investigate the correlation between lg (circSCMH1/miR-874) and acute coronary syndrome (ACS), acute myocardialinfarction (AMI), and carotid plaque stability. Methods 701 patients were divided into stable coronary artery disease (SCAD), ACS, and control groups.
Intravascular imaging (IVI), such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), play a crucial role in assessing lesion characteristics and optimizing stent placement during percutaneous coronary intervention (PCI). vs 6.7%; HR: 0.77; 95% CI: 0.61-0.97;
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). Successful PPCI was performed via right femoral artery, with access gained under ultrasound guidance.
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Am Heart J. 2000;139:430–436. Am J Cardiol.
In the subsample of patients without clinical CAD but with femoral plaque on ultrasound (n=58) who underwent cardiac computed tomography, 46% (n=27) had nonobstructive CAD and 28% (n=16) had obstructive CAD. In patients without previous CAD, but femoral plaque on ultrasound, nearly a half had nonobstructive and onefourth had obstructive CAD.
However the patient continued to have chest pain and bedside ultrasound showed hypokinesis of the septum with significantly reduced LVEF. AIVR is not always the result of significant pathology, but is classically associated with the reperfusion phase of acute myocardialinfarction. Do not treat AIVR.
If detected early by ultrasound, the patient can be saved. Our own Dave Plummer of HCMC reported on survival of 2 of 6 patients with free wall myocardial rupture diagnosed by bedside ultrasound in the ED.(3) 3) Oliva et al. (3) J Am Coll Cardiol 1995;25(5):1084-8. Armstrong PW et al. Circulation 1993;88(3):896-904.
BACKGROUND:There are limited data regarding the safety of deferral of percutaneous coronary intervention based on intravascular ultrasound (IVUS) findings. In both IVUS and FFR groups, vessels were classified into deferred or revascularized vessels, and patients were classified as those with or without deferred lesions.
Plaque regression can be demonstrated by ultrasound evaluation of the carotids which are easily accessible. Maintaining normal blood pressure also reduces the risk of stroke and myocardialinfarction. Regular exercise can bring down the blood pressure in the long run.
The problem is difficult to study because angiographic visualization of arteries is not perfect, and not all angiograms employ intravascular ultrasound (IVUS) to assess for unseen plaque or for plaque whose rupture and ulceration cannot be seen on angiogram. MINOCA I do not have the bandwidth here to write a review of MINOCA. Lindahl et al.
A pulmonary ultrasound was performed on admission and was considered positive (PE+) when there were three or more B-lines in two quadrants or more of each hemithorax. Conclusion Lung ultrasound and a high NT-proBNP (3647 ng/L in our series) on admission are the best predictors of acute heart failure needing MV in the first 48 h of ACS.
If detected early by ultrasound, the patient can be saved. Our own Dave Plummer of HCMC reported on survival of 2 of 6 patients with STEMI who had free wall myocardial rupture diagnosed by presence of hemopericardium on bedside ultrasound in the ED.(3) 3) Oliva et al. (4) J Am Coll Cardiol 1995;25(5):1084-8. Armstrong PW et al.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. Use of diuretics is strongly associated with hypokalemia and ventricular fibrillation in myocardialinfarction.
Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. RVMI explains part of the shock.
Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102). And angiographers tell me that it is sometimes difficult to say for certain based on angiogram alone, without intravascular ultrasound or, better yet, optical coherence tomography. Murakami MM.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Takotsubo is a sudden event, not one with crescendo angina. Learning Points: 1.
MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). The ways to tell for certain include intravascular ultrasound (to look for extra-luminal plaque with rupture) or "optical coherence tomography," something I am entirely unfamiliar with. I believe the latter (type II STEMI) is most likely.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) HsTnI drawn at that time was 9 ng/L (ref. 80%) and definitely too much for hour to hour. From angiography, it is not clear what the culprit is. The ECG changes were inferior, posterior, and lateral.
Smith, MD – Department of Emergency Medicine, Hennepin County Medical Center, Professor, University of Minnesota School of Medicine, Minneapolis, MN ABSTRACT: Background: Patients with type 1 myocardialinfarction with normal left ventricular function that are hemodynamically stable do not usually manifest with sinus tachycardia.
A bedside cardiac ultrasound was normal, with no effusion. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. MyocardialInfarction Type 2 and Myocardial Injury. 3–8 Shi et al.
J Cardiovasc Ultrasound. J Cardiovasc Ultrasound. Ratio of left ventricular peak E-wave velocity to flow propagation velocity assessed by color M-mode Doppler echocardiography in first myocardialinfarction: prognostic and clinical implications. Ha J et al. 2009 Sep;17(3):86-95. Park JH et al. 2011 Dec;19(4):169-73.
After rethinking the case, he remained concerned about ACS and subsequently performed a point-of-care ultrasound in order to evaluate for regional wall motion abnormality. In equivocal cases, point-of-care ultrasound may be the difference between taking the patient to the lab or not. Gray, A., & & Mills, N.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). Another approach is sympathetic chain (stellate ganglion) blockade if you have the skills to do it: it requires some expertise and ultrasound guidance.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." This was a point of care ultrasound, not a bubble contrast echo. Cath lab activated Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still.
Given her risk factors (HTN, HLD, ESRD from diabetes) I decided to obtain a broad cardiac workup for the patient: serial ECGs, labs, serial troponins, CXR and bedside cardiac ultrasound. Ultrasounds can be very helpful in guiding your diagnostic pathway: location of WMA on US led to obtaining posterior leads.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. First, the name (MyocardialInfarction or Not) is not important.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. Occlusion MyocardialInfarction (OMI) often does not present with diagnostic ST elevation, or even any STE, especially in dialysis patients.
No pericardial effusion on ultrasound." See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardialinfarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6. He had another episode the day before after exerting himself. What do you think?
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Here is the abstract: Background Identification of ST elevation myocardialinfarction (STEMI) is critical because early reperfusion can save myocardium and increase survival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content