This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The principal clinical manifestation of thrombophilia is venous thromboembolism, which is also markedly linked to arterial thrombosis, including myocardialinfarction. This report presents the case of a young man who suffered an acute myocardialinfarction as a result of thrombophilia.
Prosthetic valve thrombosis (PVT) in aortic valve and its complication coronary embolism is a very rare condition. We present a young patient with acute myocardi. Diagnosis and treatment process is challenging.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. This confirms that the pain was ischemia and is now resovled. The i nitial hs troponin I returned 75%.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. MINOCA I do not have the bandwidth here to write a review of MINOCA.
Thrombosis continues to pose a significant challenge in cardiovascular and cerebrovascular diseases, contributing to severe health complications such as myocardialinfarction, acute ischemic stroke, and venous thromboembolism. In this paper, we comment the findings reported by Liu et al.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardialinfarction (type II) and acute coronary stent thrombosis (type III). Here we share a case of Kounis syndrome type I caused by an allergy caused by a Cryptopteran bite.
COVID-19 likely increases relative risk (RR (95% CI)) of myocardialinfarction (3.3 (1.0 to 44.9)) and deep venous thrombosis (7.8 (4.3 Other RTIs also likely increase the RR of myocardialinfarction (2.9 (95% to 11.0)), stroke (3.5 (1.2 to 10)), pulmonary embolism (24.6 95% CI 1.8 to 4.9)) and stroke (2.6 (95%
Current guidelines recommend that direct anticoagulants should not be used in prevention of recurrent thrombosis in patients with antiphospholipid syndrome (APS). During a median follow-up of 53 months, we recorded venous thromboembolism (VTE), ischemic stroke or myocardialinfarction, along with major bleeding.
vs. 24.0%) Target vessel myocardialinfarction (6.4% vs 12.3%) Stent thrombosis (0.0% The study included 480 patients with ISR, finding that after one year the AGENT DCB was far superior to balloon angioplasty for… Target lesion failure (17.9% vs. 28.7%, the primary endpoint) Target lesion revascularization (12.4%
In severe OHSS, increases in capillary permeability can result in hemoconcentration and hypercoagulability leading to thrombotic events, including stroke and cerebral venous thrombosis. Within the HCUP cohort, fewer than 10 patients (<1%) were hospitalized with a stroke or thrombotic event within 60 days of OHSS diagnosis.
Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi). de Wood et al.
Bleeds were adjudicated using International Society on Thrombosis and Haemostasis criteria. Epistaxis events were less severe than nonepistaxis bleeds (International Society on Thrombosis and Haemostasis major: 3.2% Among 5247 patients with a bleeding event, 1008 (19.2%) had epistaxis and 4239 (80.8%) had nonepistaxis bleeding.
Safety outcomes included rates of symptomatic intracranial hemorrhage, parenchymal hematoma type 2, petechial hemorrhage, and in‐stent thrombosis. Similarly, the rate of in‐stent thrombosis was not significantly different between the 2 groups (1.8% 4.98];P=0.589), or petechial hemorrhage (OR, 1.11 [95% CI, 0.38–3.28];P=0.836).
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
Primary endpoint of systematic review and meta-analysis is the NACE (Net Adverse Cardiac Events) and secondary are MACE (Major Adverse Cardiac Events), mortality, bleedings, myocardialinfarction and stent thrombosis. Subgroup analyses included studies using only ticagrelor-based regimens and three-months duration of DAPT.
Adverse vascular outcomes used as endpoints include acute ischemic stroke, acute myocardialinfarction, deep vein thrombosis/pulmonary embolism, AF, and carotid artery dissection.A Patients with any adverse vascular outcomes before the index ECG were excluded. The mean age at the time of the index ECG was 44.3
A New ST-segment elevation myocardialinfarction equivalent pattern? The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardialinfarction (12.14% vs. 3.21%, (..)
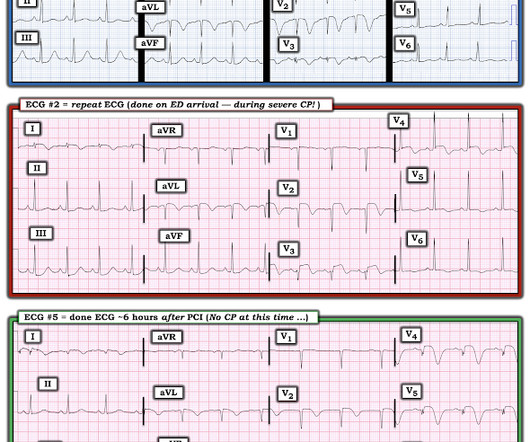
Repeat ECG while waiting for cath team, t = 56 min after arrival: It is getting worse Angiogram showed 99% acute proximal LAD thrombosis. So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5.
MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardialinfarction. 2] Driver, B.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Here is the abstract: Background Identification of ST elevation myocardialinfarction (STEMI) is critical because early reperfusion can save myocardium and increase survival.
This case provides a constellation view of the many sequelae associated with HCM – preexisting disparities of coronary perfusion due to endothelial remodeling, exacerbated diastolic dysfunction when volume depleted, conduction disorders in the diseased His-P system, and thrombosis from microvascular coronary disease. References Naidu, S.
Andreas Grüntzig, an ardent angiologist crafted an indeflatable sausage-shaped dual-lumen balloon-catheter, designed its delivery to the heart, launched minimally invasive coronary intervention and taught by beaming live demonstration. Subsequent advances are just incremental tweaks and tinkers around this fully formed framework from 1978.
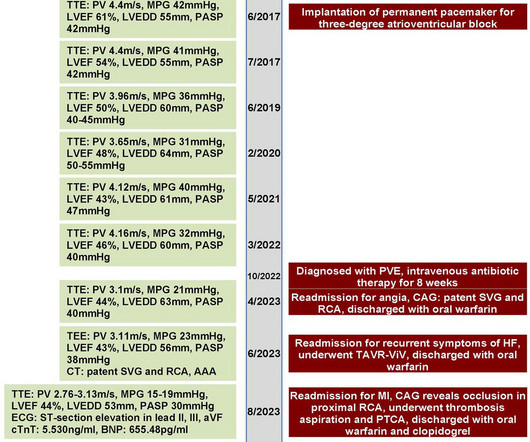
This resulted in early death due to myocardialinfarction and acute heart failure. A computed tomography revealed subclinical leaflet thrombosis. The patient was deemed unsuitable for surgery by the heart team, following which she underwent transcatheter aortic valve-in-valve replacement.
Of these, 2079 (1286 DP-DES and 793 BP-DES) met the inclusion and exclusion criteria and completed a 2-year follow-up: The primary outcome was the device-oriented composite endpoint (DOCE) of cardiac death, non-fatal target vessel myocardialinfarction and target lesion revascularisation. Results Mean age was 67 years, with 75% male.
Patients were evaluated based on a composite outcome of all-cause mortality, stroke, or myocardialinfarction. Bioprosthetic valve dysfunction (BVD) was categorized into structural valve deterioration (SVD), non-structural valve dysfunction (NSVD), clinical valve thrombosis, or endocarditis.
Patients with ST-segment–elevation myocardialinfarction undergoing primary percutaneous coronary intervention were randomly assigned by center to receive low-dose PPA or matching placebo for at least 48 hours. Circulation, Ahead of Print. mg·kg·h of bivalirudin intravenously). mg·kg·h of bivalirudin intravenously).
The ECLIPSE trial shows that use of IVI to guide coronary stenting in severely calcified lesions prevents death, stent thrombosis, and unplanned repeat procedures in this high-risk patient population. The ECLIPSE trial results were presented at the American College of Cardiology Scientific Session (ACC.25)
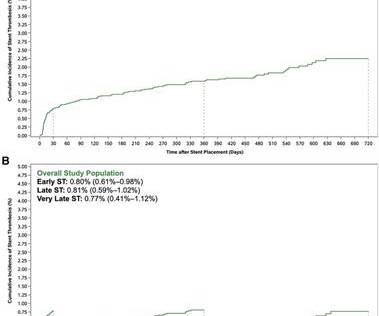
Background Stent thrombosis (ST) is an uncommon but serious complication of stent implantation. age, sex, ACS presentation, history of hypertension, smoking, diabetes, prior myocardialinfarction (MI), heart failure, prior ischemic stroke, and cancer], laboratory tests [i.e.,
The 2 coprimary outcomes were target lesion revascularization and myocardialinfarction. The secondary outcomes included ischemia-driven target lesion revascularization, target vessel myocardialinfarction, death, cardiac death, target vessel revascularization, stent thrombosis, and major adverse cardiac events.
Primary end point was a composite of ischemic stroke, myocardialinfarction, or other arterial thrombotic events. CONCLUSIONS:Intracerebral hemorrhage survivors are at high long-term risk of arterial thrombosis. Stroke, Ahead of Print. Arterial thrombotic events occurred in 169 (9.7%) patients.
vs 13.6%), any stent thrombosis (RR=1.42; 95% CI [0.35, 5.72]; p=0.62; 2.2% vs 13.6%), any stent thrombosis (RR=1.42; 95% CI [0.35, 5.72]; p=0.62; 2.2% However, FFR-guided CR showed no beneficial effect on all-cause mortality, stroke, major bleeding and myocardialinfarction.
Background Untreated multivessel disease (MVD) in acute myocardialinfarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. Similarly, all-cause mortality, cardiovascular mortality, stent thrombosis, and acute renal insufficiency did not show significant differences between two groups.
Because of the potential association of lipoprotein(a) with thrombosis, we evaluated the relationship between aspirin use and CVD events in people with elevated lipoprotein(a).Methods Due to potential confounding by indication, we matched aspirin users to nonusers using a propensity score based on CVD risk factors.
In the early years of percutaneous coronary intervention (PCI), studies indicated a heightened risk of major adverse cardiac events (MACE) in patients with reduced left ventricular ejection fraction (LVEF), involving outcomes such as death, Q-wave myocardialinfarction (MI), stent thrombosis, and repeat revascularization.
Endpoints included major adverse cardiovascular events (MACE), cardiac death, myocardialinfarction (MI), periprocedural MI, all-cause mortality, stent thrombosis (definite or probable), and target vessel revascularization (TVR). The random-effects model was used to generate risk ratios (RRs) and 95% confidence intervals (CIs).Results:A
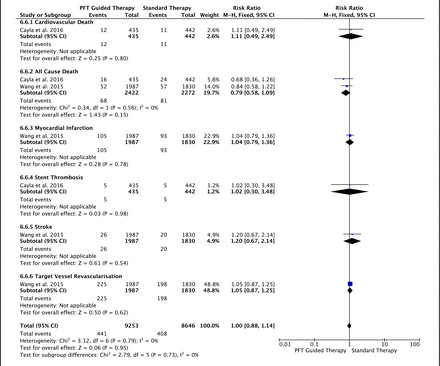
There was also no difference in the rate of bleeding between PFT-guided and standard therapies (major bleeding: RR=0.97, p=0.78, minor bleeding: RR=0.89, p=0.19 and any bleeding: RR=1.04, p=0.33).
The primary endpoint was the net clinical benefit as a composite of all-cause death, myocardialinfarction, definite or probable stent thrombosis, stroke, and major bleeding at 1 year after the index procedure in the intention-to-treat population. 0.80];P<0.001 for noninferiority;P=0.002 for superiority).
They had lower rates of mortality or myocardialinfarction. myocardialinfarction rate and 3.2% Using a side branch stent increases the risk of stent thrombosis in the main vessel and is especially to be avoided in a thrombotic situation as in acute myocardialinfarction.
Prasugrel ranked as the most efficient treatment in the composite cardiovascular efficacy outcome, all-cause death, myocardialinfarction and definite stent thrombosis, while clopidogrel ranked as safest in the bleeding outcomes. Inconsistency was moderate and non-significant (I 2 =27%, total Q p=0.2).
The primary outcome was major adverse cardiac and cerebrovascular event (MACCE), namely a composite of death from cardiovascular causes, myocardialinfarction (MI), stroke, stent thrombosis within 12 month. Patient characteristics and clinical outcomes were collected via electronic medical record system.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content