This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
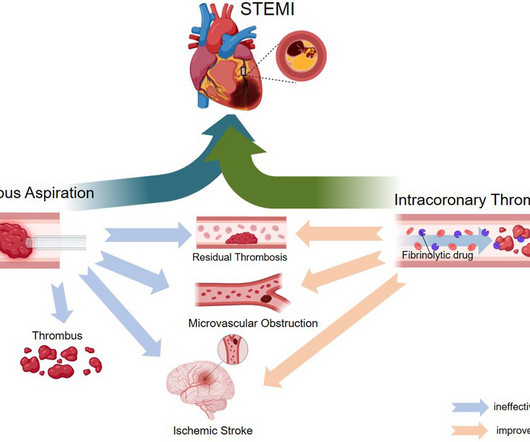
ST-elevation myocardialinfarction (STEMI) is a critical cardiovascular emergency characterized by acute coronary artery occlusion and subsequent myocardial injury. The current standard of care is primary percutaneous coronary intervention (PPCI), which aims to rapidly restore epicardial blood flow.
Background Despite restoration of epicardial blood flow in acute ST-elevation myocardialinfarction (STEMI), inadequate microcirculatory perfusion is common and portends a poor prognosis. IC thrombolysis was associated with a significantly lower incidence of MACE (RR=0.65, 95% CI 0.51 to 2.67; I 2 =25%; p<0.0001).
This case report describes a unique instance of a patient developing AEF following AF ablation, accompanied by ischemic stroke and myocardialinfarction. Upon admission, physical examination and laboratory tests revealed vital signs within abnormal ranges and indicators suggesting inflammation and potential myocardial injury.
Introduction Differences in pathophysiology, clinical presentation, and natural course of ST-elevation myocardialinfarction in female patients due to either spontaneous dissection (SCAD-STEMI) or atherothrombotic occlusion (type 1 STEMI) have been discussed. vs. 1.8 ± 5.1%, p = 0.002).
BACKGROUND:It is uncertain whether adjunctive thrombolysis is beneficial for patients with ST-segment–elevation myocardialinfarction undergoing percutaneous coronary intervention (PCI) within 120 minutes of presentation. The infarct size was detected by cardiac magnetic resonance 5 days after randomization. versus 29.0%;P<0.001)
Background Microcirculatory dysfunction is an independent risk factor for a poor prognosis after percutaneous coronary intervention (PCI) in patients with acute myocardialinfarction (AMI). Cardiac function was measured by echocardiography during hospitalization and follow-up.
The ENGAGE AF-TIMI 48 trial sought to study the safety and efficacy of edoxaban, an oral direct factor Xa inhibitor, as compared with warfarin in the treatment of atrial fibrillation.
BackgroundMicrovascular obstruction (MVO) and intramyocardial hemorrhage (IMH) are well‐established imaging biomarkers of failed myocardial tissue reperfusion in patients with ST‐segment elevation–myocardialinfarction treated with percutaneous coronary intervention. MVO and IMH were found in 299 (58%) and 182 (35%) patients.
BackgroundST-segment elevation myocardialinfarction (STEMI) persists to be prevalent in the elderly with a dismal prognosis. We assessed the Thrombolysis in MyocardialInfarction (TIMI) and Global Registry of Acute Coronary Events Risk (GRACE) scores in two groups.
BACKGROUND:T2-weighted imaging is commonly used to measure myocardial salvage in reperfused myocardialinfarction but is hindered by poor reproducibility and indistinct boundaries. The median MSI was 35.0% (interquartile range, 22.959.5%), with smaller MSI observed in patients with larger infarcts (P<0.001).
Is primary PCI superior to thrombolysis in the first hour of STEMI ? The fact of the matter is, at best, pPCI fights for equipoise in the first hour, but thrombolysis is a clear winner in moral, scientifc & holistic perspective, as it can be administered very early, at a fraction of cost ,independent of expertise and infrastructure.
In this context, we need a movement to revive the pre-hospital thrombolysis. Efficiency of thrombolysis is highly reproducible. Strategy to Reduce Mortality Rates of ST-elevation Acute MyocardialInfarction Using Prehospital Thrombolysis: A Meta-analysis. This is what CAPTIM told us. DOI: 10.4103/rcm.rcm_1_24 2.Nallamothu
The study aims to evaluate the applicability in the real world of randomised clinical trials (RCT) on antithrombotic treatment in patients with cardiovascular disease (CVD) and peripheral artery disease (PAD).
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes et al. Am Heart J.
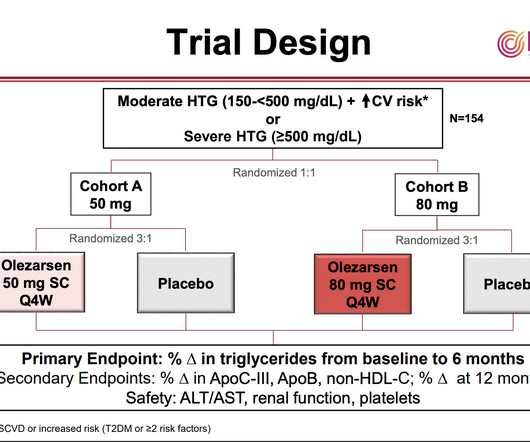
Brian Bergman, MD “Treatments to reduce high triglycerides are an unmet clinical need,” said Brian Bergmark, MD , of the Thrombolysis in MyocardialInfarction (TIMI) Study Group at Brigham and Women’s Hospital and Harvard Medical School and the study’s principal investigator.
These are the grade, TIMI grades, named after the landmark Thrombolysis In MyocardialInfarction trial. Grade 0 is no thrombus, while grade 5 is total occlusion of the vessel due to thrombus formation. Grade 0, no angiographic evidence of thrombus.
Tenecteplase (TNK) is currently being used for IV thrombolysis in acute ischemic stroke. This off-label use can lead to dosing errors related to the TNK packaging, which only states dosing for myocardialinfarction. The dosing for myocardialinfarction is 0.5 Genetech, 2023). Bach, 2023; Campbell et al.,
In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. Am Heart J (1989) 117 : pp 657-665. de Zwaan C.,
The primary efficacy outcome was a composite of acute limb ischemia, major amputation of a vascular pathogenesis, myocardialinfarction, ischemic stroke, or cardiovascular death. The principal safety end point was Thrombolysis in MyocardialInfarction major bleeding. 2.59]) with an absolute risk increase of 0.9%
The end point of interest was time to first myocardialinfarction, stroke/TIA, or coronary revascularization. We included patients with an Lp(a) measured between 1989 and 2022 and who had at least 1 year of electronic health record data before measurement of an Lp(a) level. mg/dL, of whom 23.7% had a prior cardiovascular event).
Electrocardiographic Manifestations: Acute posterior wall myocardialinfarction. Posterior myocardialinfarction: the dark side of the moon. New electrocardiographic criteria for posterior wall myocardial ischemia validated by percutaneous transluminal coronary angioplasty model of acute myocardialinfarction.
Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. Patients who received CPR or experienced reinfarction or very small infarcts due to thrombolysis also displayed Type II T-wave evolution. These do NOT indicate late, subacute MI.
Methods:STEMI patients who underwent coronary revascularization therapy and cardiac magnetic resonance (CMR) at about 4 days and 6 months between 2017 and 2023 were included.
She was diagnosed with NSTEMI with a thrombolysis in myocardialinfarction (TIMI) score of 5. Her EKG showed marked left-axis deviation, ST depressions in V2-V4, and RBBB.
Methods Inclusion and exclusion criteria of the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS), Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance (CHARISMA), Prevention of Cardiovascular events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background (..)
Acute MyocardialInfarction Due to Left Circumflex Artery Occlusion and Significance of ST-Segment Elevation. Incidence Incidence, angiographic features and outcomes of patients presenting with subtle ST-elevation myocardialinfarction. From AM, Best PJM, Lennon RJ, Rihal CS, Prasad A. Sorajja P, Gersh BJ, Cox DA, et al.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. Impact of total occlusion of culprit artery in acute non-ST elevation myocardialinfarction: a systematic review and meta-analys is.
The TIMI (Thrombolysis in MyocardialInfarction) Study Group is a Division of Cardiovascular Medicine at the esteemed Brigham and Women’s Hospital and Harvard Medical School. Anish Koka, MD @anish_koka This was driven almost entirely by myocardialinfarction / need for revascularization.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. Incidence of an acute coronary occlusion. Am J Med 2019, 132(5):622-630. link] Harhash AA et al.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. In the setting of evolving infarction — development of AIVR often heralds the onset of reperfusion ( following thrombolysis, acute angioplasty, or spontaneous reperfusion ).
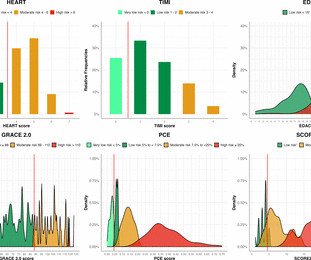
Background Guidelines recommend the use of risk scores to select patients for further investigation after myocardialinfarction has been ruled out but their utility to identify those with coronary artery disease is uncertain. The negative predictive value (NPV) varied from 77.3% –100%).
Initial diagnostics indicated non-ST-elevation myocardialinfarction, leading to immediate intervention. A combination of balloon angioplasty, stent implantation, and intra-arterial thrombolysis with recombinant tissue plasminogen activator (rt-PA) was employed, resulting in significant thrombus reduction and improved coronary flow.
ECG #3 is easily recognized as OMI and the AI model recommends immediate revascularization The patient in today's case received suboptimal care and suffered a substantial myocardialinfarction. Here is evidence for this: Opiates are associated with worse outcomes in MyocardialInfarction. Abstract 556.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J 2000;139(3):4306.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content