This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
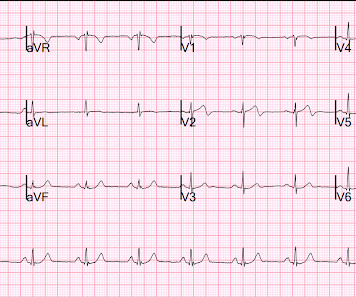
76-year-old man, with a history of inferior wall myocardialinfarction. In this ECG, at the beginning, the last part of a wide-complex tachycardia is visible. After 2 sinus beats, another wide-complex tachycardia begins (with the same QRS configuration).
A multicenter study has described and validated a new strategy for guiding ablation procedures in patients with complex tachycardias. This type of procedure is frequently used to treat ventricular tachycardias originating in areas affected by scarring after a myocardialinfarction.
If a wide complex tachycardia occurs, the probability is very high that it is a ventricular tachycardia (approx. 80%, in patients with a previous myocardialinfarction (.) Here we see a broad complex tachycardia that looks like an RBBB + LAFB, which is regular. In this constellation, 3 causes must be considered: 1.
Regular tachycardia (124 beats per min), diaphoresis, and rales were present. A 69-year-old man with a history of MI and cardiomyopathy presented with 2 days of dyspnea. A diagnosis was made.
Broad complex tachycardia in a 78-year-old patient with coronary heart disease (CHD) and an old inferior myocardialinfarction. Why is this a ventricular tachycardia (VT) and not a supraventricular tachycardia (SVT) with aberrant conduction? What other clues are there?
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
If a wide complex tachycardia occurs, the probability is very high that it is a ventricular tachycardia (approx. 80%, in patients with a previous myocardialinfarction (.) Here we see a broad complex tachycardia that looks like an RBBB + LAFB, which is regular. In this constellation, 3 causes must be considered: 1.
A 64-year-old male with recurrent ventricular tachycardia (VT) was referred for repeat ablation. His medical history included prior myocardialinfarction and cardiac magnetic resonance imaging demonstrated basal inferior and anteroseptal subendocardial scar with overall preserved left ventricular function.
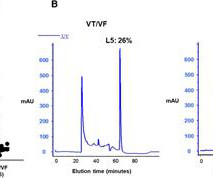
Background Early ventricular tachycardia/fibrillation (VT/VF) in patients with ST-elevation myocardialinfarction (STEMI) has higher morbidity and mortality. This study examines gender-differentiated risk factors and underlying mechanisms for early onset VT/VF in STEMI.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. Hammill SC. Edwards WD.
The principal clinical manifestation of thrombophilia is venous thromboembolism, which is also markedly linked to arterial thrombosis, including myocardialinfarction. This report presents the case of a young man who suffered an acute myocardialinfarction as a result of thrombophilia.
Three or more ventricular beats in a row at a rate above 100 per minute is termed ventricular tachycardia. Ventricular tachycardia lasting more 30 seconds or requiring termination earlier due to hemodynamic compromise is called sustained ventricular tachycardia. Either case, the treatment is ablation of the right bundle.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Mapping data in post-myocardialinfarction (MI) patients describe ventricular tachycardia (VT) re-entry circuits of slow VT, that are typically related to transmural scars. Fast VTs with cycle lengths close to the refractory period may be related to functional re-entry in the scar border zone (BZ).
Alternatively , it is someone who has an old myocardialinfarction and is now very sick with something else. The patient spontaneously converted back to sinus tachycardia. They agreed that the ECG findings were due only to old MI and tachycardia. Later, I obtained more clinical history. Looks like atrial fibrillation.
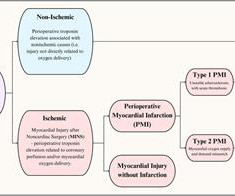
Perioperative myocardial injury is a relatively common complication after noncardiac surgery associated with significant morbidity and mortality. It is frequently driven by physiologic factors such as hypotension, tachycardia, and anemia.
The activation signal, or signature, defined as the cumulative number of recording sites that have activated per millisecond, was utilized to segment each re-entrant ventricular tachycardia (VT) circuit into inner and outer circuit pathways, and as an estimate of best ablation lesion location to prevent VT.
The tachycardia was gone by the time paramedics arrived. He was unconscious for 8 minutes and slowly awoke in the ambulance, complaining of nausea only. First responders found him to be very tachycardic , confused, perserverating and with no memory of the event. There was tongue biting. Lightheadedness continued. Interpretation.
This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. There is widespread ST depression. Figure-1: Comparison of the first 2 ECGs in today's case.
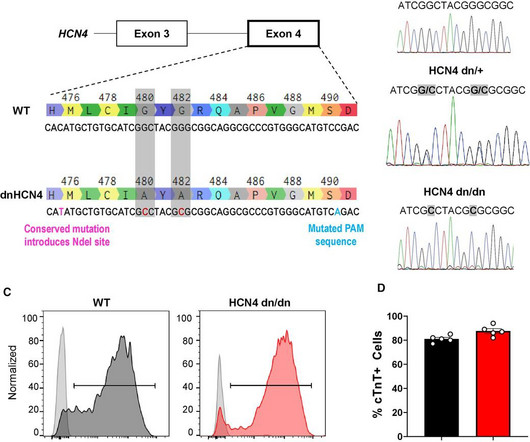
BackgroundHuman pluripotent stem cell-derived cardiomyocytes (hPSC-CMs) show tremendous promise for cardiac regeneration following myocardialinfarction (MI), but their transplantation gives rise to transient ventricular tachycardia (VT) in large-animal MI models, representing a major hurdle to translation.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Supraventricular tachycardia – more than 7 consecutive complexes of supraventricular beats at a rate of > 100 bpm.
Different imaging modalities have been used to image and display scar tissue accelerating substrate identification and streamlining mapping and ablation of ventricular tachycardias (VTs). Cardiac magnetic resonance imaging (CMR) is referred as the gold standard for identifying scar tissue especially after myocardialinfarction or injury1.
In that study commonest ECG abnormalites were QTc prolongation followed by brady/tachycardia and then ST segment deviations [3]. ECG changes resembling ST elevation myocardialinfarction has also been described after traumatic intracranial hemorrhage [4]. In a study of 204 subjects, 31% had troponin elevation. N Engl J Med.
The classical view that scarred, fibrotic myocardium in patients with myocardialinfarction (MI) is the basis for ventricular tachycardia by producing a critical activation delay in surviving myocardial strands1 was recently challenged by Sung et al.2
The ECG is diagnostic of occlusion myocardialinfarction (OMI). I would have favored emergent coronary CT angiogram had I cared for this patient. == Learning points: Diagnosis of occlusion myocardialinfarction (OMI) can be extremely difficult and takes time and effort to learn well.
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenic shock or 2 simultaneous pathologies. Here is that ECG: What do you think? See Table for diagnostic utility.
Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. But we are now concerned with the precordial leads. BP was 160/100.
There is sinus tachycardia. Because of the high troponin, echocardiography was done and showed a wall motion abnormality in the anterior, anterolateral, and apical walls, consistent with LAD myocardialinfarction. I saw this as I was reading a large a stack of ECGs: What do you think? The QTc is 462 ms. It was stented.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. Breath sounds were clear in all lung fields. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily.
ECG in a person with persistent anginal pain for the past several hours showing significant ST segment depression anterolateral leads along with sinus tachycardia. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardialinfarction.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Here is the abstract: Background Identification of ST elevation myocardialinfarction (STEMI) is critical because early reperfusion can save myocardium and increase survival.
Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis? The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. If it is MI, is it type 1 or type 2? Is it STEMI or NonSTEMI? Is it acute persistent occlusion?
The important point for our purposes is that they do no represent myocardialinfarction. T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. Dr. Smith note: I wouldn't necessarily consider this ENTIRELY "benign." Indeed, they have a higher incidence of structural problems. What is it?
IntroductionAcute coronary syndrome refers to a group of diseases characterized by sudden, decreased blood supply to the heart muscle that results in cell death, also known as acute myocardialinfarction. The majority of patients (67.9%) have been diagnosed with ST- Elevated MyocardialInfarction and were classified as Killip class I.
I do not think this is acute occlusion myocardialinfarction (OMI). I learned more about the history: 30-something African American with 5-7days of sharp R-sided shoulder/scapula/chest discomfort, presented with sinus tachycardia. Get an emergent contrast echocardiogram. These are reasons why it does not look like OMI: 1.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. That said, against acute PE — is the inconstancy of this patient's symptoms — the lack of tachycardia — and the lack of any other ECG signs of acute RV strain.
In addition to sinus tachycardia, the only abnormalities listed by the computer were "low voltage, precordial leads" and "anteroseptal infarct, old.Q Next trop 85,528 ng/L (consistent with a massive myocardialinfarction), none further measured. 4) There is well formed J-point notching. Case 2: What do you think?
Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk. In such cases, it is common for tachycardia to exaggerate the ST Elevation And, in fact, there was no new acute MI at this visit - troponins did not rise again. Murakami M. Acute Cardiovascular Care 2014;3(4):317-325.
myocardialinfarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. Hypotension may of course be a result of a brady- or tachydysrhythmia. 2) Hypoxia, including poisons of oxidative phosphorylation such as HS, CO, CN. Fundamentally, cardiogenic shock is an issue of decreased cardiac output.
Then, why is it mentioned that, implanting a defibrillator soon after an acute myocardialinfarction, in those with left ventricular dysfunction and prone for ventricular arrhythmias and sudden cardiac death, is not useful? Then, why is it mentioned that, an implantable defibrillator, is not useful, soon after myocardialinfarction?
Sympathetic nervous system hyperactivity plays a major role in the pathogenesis of ventricular arrhythmias following myocardialinfarction (MI).1,2 1,2 The stellate ganglia are an important nexus point for sympathetic innervation to the heart.3
Background:Ischemia-related ventricular arrhythmia is the leading cause of death in patients after acute myocardialinfarction (AMI). To test the ventricular arrhythmogenesis post-AMI, we measured ventricular tachycardia/fibrillation (VT/VF) from 24-hour telemetry ECG recording in conscious rats.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content