This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Suddencardiacdeath (SCD) risk stratification is based on clinically recognized risk factors (RF), such as reduced left ventricular (LV) ejection fraction (EF), heart failure (HF), prior myocardialinfarction (MI), and syncope. These RFs fail to capture the majority of SCDs.
SCAD can cause acute coronary syndrome and myocardialinfarction (MI), as well as suddencardiacdeath. Spontaneous coronary artery dissection (SCAD) is an uncommon condition which is increasingly recognized as a cause of significant morbidity.
Does use of left ventricular ejection fraction (LVEF) and/or other variables identify patients who benefit from defibrillator implantation to prevent suddendeath after acute myocardialinfarction (MI)?
ConclusionsARBBB is a predictor of inhospital SCD, CR, and 2year major adverse cardiovascular and cerebrovascular events in patients with firstepisode acute myocardialinfarction undergoing percutaneous coronary intervention with a drugeluting stent.
Then, why is it mentioned that, implanting a defibrillator soon after an acute myocardialinfarction, in those with left ventricular dysfunction and prone for ventricular arrhythmias and suddencardiacdeath, is not useful? Mostly for protection against suddencardiacdeath. That is one reason.
Sympathetic nervous system hyperactivity plays a major role in the pathogenesis of ventricular arrhythmias following myocardialinfarction (MI).1,2 1,2 The stellate ganglia are an important nexus point for sympathetic innervation to the heart.3
Understanding the difference between heart attack and cardiac arrest can help in recognizing symptoms, seeking prompt medical care, and even saving lives. A heart attack, or myocardialinfarction, happens when an artery becomes blocked, reducing blood flow to the heart muscle. What is a Heart Attack?
Suddencardiacdeath (SCD) is one of the most important causes of mortality in the world. Myocardialinfarction (MI) is a major risk factor for SCD associated with significant pro-arrhythmic structural and electrophysiological ventricular remodelling.
Morbidity and mortality rates after MyocardialInfarction (MI) remain high despite advancements in therapy. Post-MI cardiac remodeling leads to heart failure and electrical aberrancies which result in lethal arrhythmias and suddencardiacdeath.
The incidence of myocardialinfarction (MI) and suddencardiacdeath (SCD) is significantly higher in individuals with Type 2 Diabetes Mellitus (T2DM) than in the general population. Strategies for the prevent.
Implantable cardiac defibrillator (ICD) implantation can protect against suddencardiacdeath (SCD) after a myocardialinfarction. However, improved risk stratification for device requirement is still needed.
There is an unmet need for better risk stratification for suddencardiacdeath in the era of primary prevention ICD therapy. Scar burden on LGE-CMR imaging may be a risk marker for ventricular arrhythmia post-myocardialinfarction (MI).
The main result of the CAST (Cardiac Arrhythmia Suppression Trial), shown in Figure 1,1 was completely unexpected: The suppression of ventricular ectopy with antiarrhythmic drugs (AADs) was associated with an increased incidence of lethal ventricular arrhythmias in patients with post–myocardialinfarction (post-MI) at high risk of suddencardiacdeath (..)
Participants were monitored for three primary endpoints: a relapse necessitating revascularization, or another procedure to restore blood flow in the blocked artery; myocardialinfarction, or a heart attack caused by lack of blood flow to the heart; and suddencardiacdeath. percent).
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of suddencardiacdeath in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%. vs 19.1%, p<0.0001) and myocardialinfarction (56.1%
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chest pain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardialinfarction, ventricular arrhythmia and suddencardiacdeath.
Furthermore, there was no family history of early CAD, MI, or suddencardiacdeath. The peak Troponin I confirmed myocardialinfarction. (A Posterior myocardialinfarction: The dark side of the moon. The delayed action wave in non-ST-elevation myocardialinfarction. 1] Driver, B.
Transcript of the video: Brugada Syndrome was described by Brugada brothers in 1992 as right bundle branch block pattern in anterior leads with ST segment elevation and syncope or suddencardiacdeath and it was later in 1998, that the genetic basis of the disease was identified, with mutations in sodium channel.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4
The TIMI (Thrombolysis in MyocardialInfarction) Study Group is a Division of Cardiovascular Medicine at the esteemed Brigham and Women’s Hospital and Harvard Medical School. Importantly, there was no difference in cardiovascular death or death from any cause.
In most cases, rather, the culprit is gross ischemia due to myocardialinfarction, cardiomyopathy, or advanced coronary artery disease. Pleomorphic ventricular tachycardia and risk for suddencardiacdeath. genes implicated in congenital Long QT syndrome, such as SCN5A and KCNQ1). [1-3, 8] Liu, E.,
This also confirms right ventricular infarction (RV MI) A follow up TTE demonstrated a normal LVEF with a “regional wall motion abnormality-posterolateral hypokinetic mild, probable.” He has a history of suddencardiacdeath in his family. His troponin I peaked at 6.107 ng/mL. Learning Points : 1.
AF is associated with an increased risk of death as well as multiple adverse outcomes, including stroke, cognitive impairment or dementia, myocardialinfarction, suddencardiacdeath, heart failure (HF), chronic kidney disease (CKD), and peripheral artery disease (PAD). million.
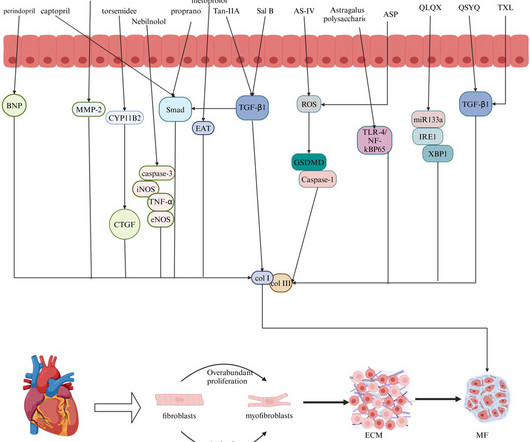
Myocardial fibrosis (MF) is a common pathological manifestation of many cardiovascular diseases, such as myocardialinfarction, myocardial ischemia, and suddencardiacdeath.
Adding TXL to WM showed a non-significant trend toward reducing myocardialinfarction [RR 0.34, 95% CI (0.05, 2.12); NNT=41] and suddencardiacdeath [RR 0.34, 95% CI (0.01, 8.28); NNT=65]. No increase in adverse events was observed when TXL was added to WM [RR 1.02, 95% CI (0.70, 1.49); NNT=149].ConclusionsOur
The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Acute myocardialinfarction triggered by emotional stress.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content