This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Drug-eluting stents (DESs) have become the gold standard of coronary angioplasty since their inception in 2002. vs 57.5%, p=0.010), a greater average number of stents implanted per patient (1.72±0.92 vs 57.5%, p=0.010), a greater average number of stents implanted per patient (1.72±0.92
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
The 2 coprimary outcomes were target lesion revascularization and myocardialinfarction. The secondary outcomes included ischemia-driven target lesion revascularization, target vessel myocardialinfarction, death, cardiac death, target vessel revascularization, stentthrombosis, and major adverse cardiac events.
Patients with ST-segment–elevation myocardialinfarction undergoing primary percutaneous coronary intervention were randomly assigned by center to receive low-dose PPA or matching placebo for at least 48 hours. Circulation, Ahead of Print. mg·kg·h of bivalirudin intravenously). mg·kg·h of bivalirudin intravenously).
Background Bioresorbable vascular scaffolds (BVS) were designed to reduce the rate of late adverse events observed in conventional drug-eluting stents (DES) by dissolving once they have restored lasting patency.
Drug‐eluting stents have been shown to be superior to bare‐metal stents in patients with HBR, even when patients were given abbreviated periods of dual antiplatelet therapy (DAPT). Short DAPT has not been evaluated with the EluNIR ridaforolimus‐eluting stent. presented with acute coronary syndrome; 33.7%
Background For high bleeding-risk patients (HBR) undergoing percutaneous coronary intervention (PCI), the LEADERS FREE (LF) and LEADERS FREE II (LF II) trials established the safety and efficacy of a stainless steel polymer-free biolimus-coated stent (SS-BCS) with 30 days of dual antiplatelet treatment (DAPT).
Background:Stopping aspirin within 1 month after implantation of a drug-eluting stent (DES) for ticagrelor monotherapy has not been exclusively evaluated for patients with acute coronary syndrome (ACS). Circulation, Ahead of Print. 0.80];P<0.001 for noninferiority;P=0.002 for superiority). versus 3.4%; HR, 0.35 [95% CI, 0.20–0.61];P<0.001).Conclusions:This
vs 13.6%), any stentthrombosis (RR=1.42; 95% CI [0.35, 5.72]; p=0.62; 2.2% vs 13.6%), any stentthrombosis (RR=1.42; 95% CI [0.35, 5.72]; p=0.62; 2.2% However, FFR-guided CR showed no beneficial effect on all-cause mortality, stroke, major bleeding and myocardialinfarction.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardialinfarction (type II) and acute coronary stentthrombosis (type III). Here we share a case of Kounis syndrome type I caused by an allergy caused by a Cryptopteran bite.
Background Untreated multivessel disease (MVD) in acute myocardialinfarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. Similarly, all-cause mortality, cardiovascular mortality, stentthrombosis, and acute renal insufficiency did not show significant differences between two groups.
3.30]) and subacute definite or probable stentthrombosis (0.58% and 0.17%; hazard ratio, 3.40 [95% CI, 1.26–9.23]) years; men, 76.6%; acute coronary syndrome, 75.0%). There was no difference in net adverse clinical outcomes and each component of coprimary cardiovascular end point.
The United States has been way behind other nations in using drug-coated balloons (DCB) to treat coronary in-stent restenosis (ISR), but that’s about to change thanks to the FDA approval of Boston Scientific’s AGENT Drug-Coated Balloon. vs. 24.0%) Target vessel myocardialinfarction (6.4% vs 12.3%) Stentthrombosis (0.0%
If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. Since the FFR wire can be used for guiding balloon catheters and stents, it is easy to make post procedure measurements without any additional effort. Routine FFR measurement probably lead to more judicious use of stents and improved outcomes.
BackgroundProcedural intravenous cangrelor has been proposed as an effective platelet inhibition strategy for stenting in acute ischemic stroke. Safety outcomes included rates of symptomatic intracranial hemorrhage, parenchymal hematoma type 2, petechial hemorrhage, and in‐stentthrombosis. 3.28];P=0.836). versus 0%;P=0.911).ConclusionCangrelor
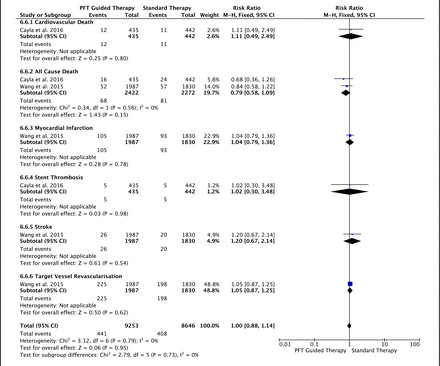
There was also no difference in the rate of bleeding between PFT-guided and standard therapies (major bleeding: RR=0.97, p=0.78, minor bleeding: RR=0.89, p=0.19 and any bleeding: RR=1.04, p=0.33).
In the early years of percutaneous coronary intervention (PCI), studies indicated a heightened risk of major adverse cardiac events (MACE) in patients with reduced left ventricular ejection fraction (LVEF), involving outcomes such as death, Q-wave myocardialinfarction (MI), stentthrombosis, and repeat revascularization.
The near-immediate or instant feedback learning process by which the heart responds to any new invasive procedural variation facilitates each new change; be it drug-eluting stent, drug-coated balloon, or both in different combinations and permutations.
The primary outcome was major adverse cardiac and cerebrovascular event (MACCE), namely a composite of death from cardiovascular causes, myocardialinfarction (MI), stroke, stentthrombosis within 12 month. Patient characteristics and clinical outcomes were collected via electronic medical record system.
Prasugrel ranked as the most efficient treatment in the composite cardiovascular efficacy outcome, all-cause death, myocardialinfarction and definite stentthrombosis, while clopidogrel ranked as safest in the bleeding outcomes. Inconsistency was moderate and non-significant (I 2 =27%, total Q p=0.2).
Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi). It was stented.
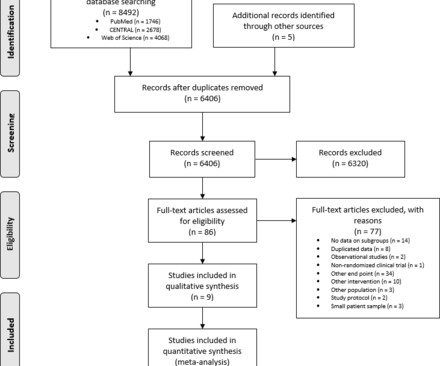
Primary endpoint of systematic review and meta-analysis is the NACE (Net Adverse Cardiac Events) and secondary are MACE (Major Adverse Cardiac Events), mortality, bleedings, myocardialinfarction and stentthrombosis. A total of eight studies and 12,665 patients were included in our analysis.
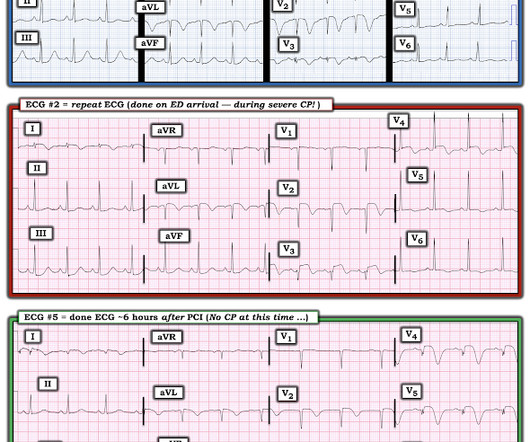
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. A New ST-segment elevation myocardialinfarction equivalent pattern? An Impella was placed for cardiac output augmentation.
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). The primary non-inferiority endpoint was MACCE (a composite of cardiac death, MI, ischaemic stroke, stentthrombosis, or target vessel revascularisation). in the medical therapy group. Atlanta, GA.
Repeat ECG while waiting for cath team, t = 56 min after arrival: It is getting worse Angiogram showed 99% acute proximal LAD thrombosis. It was opened and stented. The Cath lab was activated. Peak trop > 50,000 ng/L Formal Bubble contrast echo Severe LV systolic dysfunction.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement. References 1] Smith, S.
It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. Acute myocardialinfarction in patients with dialysis Patients on dialysis have a well studied history of underdiagnosis and undertreatment for acute myocardialinfarction. What can we learn?
A mid-LAD culprit lesion was identified and stented. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution. References Naidu, S. American College of Cardiology.
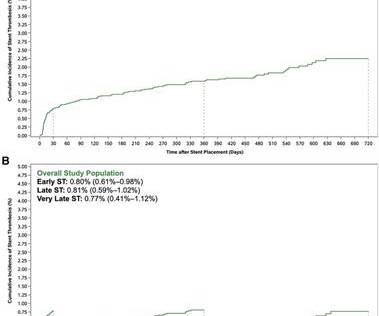
Background Stentthrombosis (ST) is an uncommon but serious complication of stent implantation. Methods The analysis included patients who received stent placement for the index acute coronary syndrome (ACS). drug-eluting stent (DES) vs. bare-metal stent (BMS) and anticoagulant with rivaroxaban vs. placebo].
IntroductionThe simultaneous occurrence of acute myocardialinfarction (AMI) and venous thromboembolism (VTE) is rare and often associated with underlying malignancies. Subsequent investigations revealed pulmonary embolism, deep vein thrombosis, and imaging findings suggestive of pancreatic cancer.
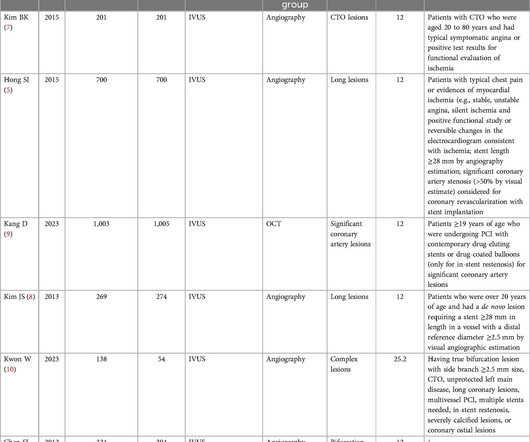
We included major adverse cardiovascular events (MACE), myocardialinfarction (MI), cardiac death and other outcome indicators. ConclusionsCompared with the non-IVUS-guided group, IVUS-guided stent implantation may be more effective for patients with complex CAD.Systematic Review RegistrationPROSPERO [CRD42024531366].
History of diabetes type II and stent placement in 2018. Let's see how the PMCardio Queen of Hearts AI Model performs: "Acute Occlusive MyocardialInfarction" She gave this a score of 1.0 (100% This was texted to me by a paramedic while I was out running one day: "54 yo male chest pain started at 1pm. What do you think?
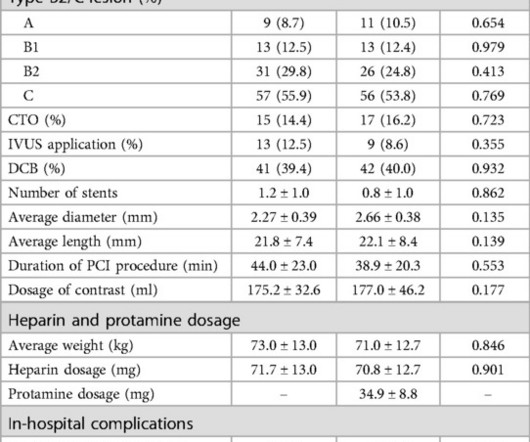
In group II, circulating heparin was neutralized with a half dose of protamine sulfate, and the brachial sheath was removed immediately after the procedure.ResultsThere were no cases of acute stentthrombosis, nonfatal myocardialinfarction or in-hospital mortality in either group.
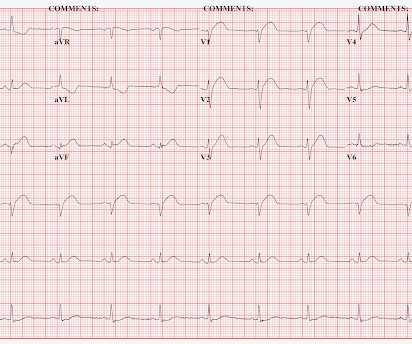
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content