This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
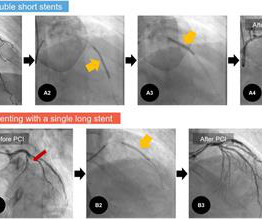
Objectives There is no consensus regarding the optimal choice between single long stent (SLS) and overlapped double short stents (DSS) in patients with acute myocardialinfarction (AMI). Therefore, we aimed to compare treatment outcomes among patients with AMI treated with these two different stenting methods.
(MedPage Today) -- For the first time, intravascular imaging-guided coronary stenting was associated with better survival and reduced myocardialinfarction (MI) in a meta-analysis powered to detect these benefits against angiography, researchers.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Smith: This is an enormous myocardialinfarction. This was stented with a 2.25 Next trop in AM.
(MedPage Today) -- As a stricter gatekeeper to nonculprit lesion intervention in people with acute myocardialinfarction (MI) going for complete revascularization, fractional flow reserve (FFR) guidance was projected to save medical costs and increase.
He underwent coronary stenting (uncertain which artery). He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. I do not have the post-resuscitation ECG. He underwent months of rehabilitation and was able to return to work part time. Could this have been avoided?
Clinical success was defined as optimal stent expansion after final treatment with no in-hospital major adverse cardiovascular event (MACE). stent expansion at Maximum Calcium Site 96.7% stent expansion at Maximum Calcium Site 96.7% Clinical Safety and Effectiveness Results: - 98.3%
So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). So I made an ED diagnosis of Non-Occlusion MyocardialInfarction (NOMI), and his next day angiogram confirmed NOMI.
Publication date: Available online 4 March 2024 Source: The American Journal of Cardiology Author(s): Sanjit S. Jolly, Shun Fu Lee, Rajibul Mian, Sasko Kedev, Shahar Lavi, Raul Moreno, Gilles Montalescot, Ali Hillani, Timothy D. Henry, Valon Asani, Robert F. Storey, Johanne Silvain, James C.S.
So we know there is myocardialinfarction and the patient has persistent pain, but it is very mild. The culprit was opened and stented. Only the ECG and presence or absence of pain can tell you what is happening right now. Again , I would give NTG and re-assess. Case continued: A 2nd troponin I returned at 744 ng/L.
She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. Hyperacute T Wave in the Early Diagnosis of Acute MyocardialInfarction. Interpretation of acute myocardialinfarction with persistent “hyperacute T waves” by cardiac magnetic resonance. 2023;82:194–202.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. Only when the first troponin (high sens trop I) returned at around 22,000 ng/L did the cardiologist reconsider. Peak troponin was not recorded.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardialinfarction (type II) and acute coronary stent thrombosis (type III). Here we share a case of Kounis syndrome type I caused by an allergy caused by a Cryptopteran bite.
Background:Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are two types of carotid revascularization procedures performed on symptomatic patients. Stroke, Volume 56, Issue Suppl_1 , Page ATP229-ATP229, February 1, 2025. This data provides further insight into the risks involved in carotid revascularization procedures.
The near-immediate or instant feedback learning process by which the heart responds to any new invasive procedural variation facilitates each new change; be it drug-eluting stent, drug-coated balloon, or both in different combinations and permutations.
The United States has been way behind other nations in using drug-coated balloons (DCB) to treat coronary in-stent restenosis (ISR), but that’s about to change thanks to the FDA approval of Boston Scientific’s AGENT Drug-Coated Balloon. vs. 24.0%) Target vessel myocardialinfarction (6.4% vs 12.3%) Stent thrombosis (0.0%
Electrocardiographic Criteria to Differentiate Acute Anterior ST Elevation MyocardialInfarction from Left Ventricular Aneurysm. Former resident: "Just saw cath report, LAD stent was 100% acutely occluded." They of course opened and stented it. American Journal of Emergency Medicine 2005; 23(3):279-287.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). Additional arterial access via left brachial artery was obtained, and a covered stent was deployed successfully in the right femoral artery with satisfactory haemostasis.
Just before 10 AM, the patient received a stent to the culprit OM. Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). Peak troponin was 12 ng/mL. & Griffin, J. link] Lee, T.
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardialinfarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
In this study, we evaluate the safety and efficacy of TCAR in patients with symptomatic internal carotid artery disease compared with carotid endarterectomy (CEA) and carotid artery stenting (CAS).METHODS:A The primary outcomes included a 30-day stroke or transient ischemic attack, myocardialinfarction, and mortality.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. He had no h/o heart failure. DBT was 120 minutes, pretty good for a Non-STEMI OMI.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. The patient was transferred to CCU to consider surgical options. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
A stent was placed. In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. de Zwaan C., Wellens H.J.J.,
Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L. Previously placed stents in the LAD (multiple) and mid circumflex and patent Formal echocardiogram: Normal left ventricular size and wall thickness.
BackgroundProcedural intravenous cangrelor has been proposed as an effective platelet inhibition strategy for stenting in acute ischemic stroke. Safety outcomes included rates of symptomatic intracranial hemorrhage, parenchymal hematoma type 2, petechial hemorrhage, and in‐stent thrombosis. 3.28];P=0.836). versus 0%;P=0.911).ConclusionCangrelor
Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) and Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) integer scoring systems were tested.
An open 90% LAD was stented. Here is the ECG the next AM: There was so little infarction that there are lateral, but no anterior reperfusion T-waves (normally, there would be Wellens' type waves after LAD reperfusion). Here is some older but very interesting literature on TIMI myocardial perfusion grade and ST resolution : 1.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. A New ST-segment elevation myocardialinfarction equivalent pattern? An Impella was placed for cardiac output augmentation.
Patients in the combination AP +AC therapy group had a higher prevalence of CAD, myocardialinfarction, and coronary/vascular stent placement compared to the AC monotherapy group. The median follow-up of patients was 57 months. The median follow-up of patients was 57 months.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions.
The ECG is diagnostic of occlusion myocardialinfarction (OMI). This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP. Patient #3 — turned out to have myocarditis.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. Such an escape would have a wider complex.
The primary outcomes included 30-day combined stroke and transient ischemic attack (TIA), myocardialinfarction (MI), and mortality. This was explained in Figure 1.Results:A Results:A total of seven studies involving 24,246 patients were analyzed. 1.82), and MI (OR:1.29,95%CI:0.83-2.01) 2.01) but lower mortality (OR:0.42,95%CI:0.22-0.81).
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. At that visit the patient was found to have an in-stent RCA occlusion. She's had multiple PCI procedures. Troponin I peaked at 18.323ng/L.
Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102). This was a presumed culprit and a stent was placed. The only study I'm aware of that looked at this was mine, in which 4% of Type II MI had New ST Elevation. Murakami MM.
The OM-1 was opened and stented, then the LAD was stented 3 days later. The acute infarct-related artery was off the circumflex and the affected wall was posterior (STEMI). The LAD had a 75% proximal lesion that by fractional flow reserve was hemodynamically significant. The posterior leads were falsely negative.
Primary endpoint of systematic review and meta-analysis is the NACE (Net Adverse Cardiac Events) and secondary are MACE (Major Adverse Cardiac Events), mortality, bleedings, myocardialinfarction and stent thrombosis. Subgroup analyses included studies using only ticagrelor-based regimens and three-months duration of DAPT.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. All three lesions had TIMI 2 flow prior to stenting. Because: 1) He has been reading this blog for a long time.
Because of the high troponin, echocardiography was done and showed a wall motion abnormality in the anterior, anterolateral, and apical walls, consistent with LAD myocardialinfarction. It was stented. Had it not opened on its own, it could have resulted in a very large anterior wall MI.
Elevated Lp(a) concentrations in patients with ischaemic heart disease have been linked to higher rates of peri-procedural myocardialinfarction (MI) during percutaneous coronary intervention (PCI).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content