This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He underwent coronary stenting (uncertain which artery). An emergency cardiac ultrasound could be very useful. He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. I do not have the post-resuscitation ECG. Could this have been avoided?
But there are also new Q-waves, stronly suggesting new infarction. A bedside cardiac ultrasound performed by a true EM expert (Robert Reardon, who wrote the cardiac ultrasound chapter in Ma and Mateer) showed an inferior wall motion abnormality. The culprit was opened and stented. Again , I would give NTG and re-assess.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). Successful PPCI was performed via right femoral artery, with access gained under ultrasound guidance.
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Am Heart J. 2000;139:430–436. Am J Cardiol.
Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102). This was a presumed culprit and a stent was placed. The only study I'm aware of that looked at this was mine, in which 4% of Type II MI had New ST Elevation. Murakami MM.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions.
Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Posterior wall involvement attenuates predictive value of ST-segment elevation in lead V4R for right ventricular involvement in inferior acute myocardialinfarction.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." This was a point of care ultrasound, not a bubble contrast echo. Cath lab activated Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still.
Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion MyocardialInfarctions. A single DES stent was placed, and the patient did well post-procedure. Academic Emergency Medicine 27(S1): S220. Abstract 556. Most other arteries had scattered 20-30% stenoses.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. After many hours, the decided that it was appropriate to do an angiogram and they found a distal LAD occlusion which was opened and stented. It was stented. There was no wall motion abnormality.
The 2 coprimary outcomes were target lesion revascularization and myocardialinfarction. The secondary outcomes included ischemia-driven target lesion revascularization, target vessel myocardialinfarction, death, cardiac death, target vessel revascularization, stent thrombosis, and major adverse cardiac events.
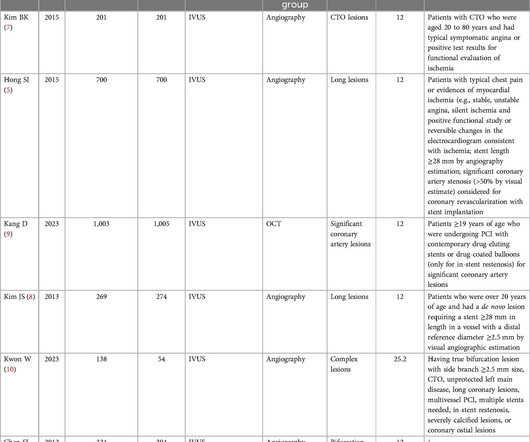
Introduction Intravascular ultrasound (IVUS) improves clinical outcome in patients undergoing percutaneous coronary intervention (PCI) but dedicated prospective studies assessing the safety and efficacy of IVUS guidance during primary PCI are lacking.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. This was stented. Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. Patients with acute myocardialinfarction and a potassium level of less than 4.0
Intravascular imaging (IVI), such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), play a crucial role in assessing lesion characteristics and optimizing stent placement during percutaneous coronary intervention (PCI). vs 6.7%; HR: 0.77; 95% CI: 0.61-0.97;
After rethinking the case, he remained concerned about ACS and subsequently performed a point-of-care ultrasound in order to evaluate for regional wall motion abnormality. He was successfully treated with one drug eluting stent. A second troponin had been drawn 3 hours after arrival and was again less than 0.30ng/mL. Gray, A., &
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. There was initially TIMI 0 flow.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. It was stented. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5,
They did not have an ultrasound on the ambulance (some local crews are starting to utilize POC limited US in our service areas). He was successfully stented. Posterior wall involvement attenuates predictive value of ST-segment elevation in lead V4R for right ventricular involvement in inferior acute myocardialinfarction.
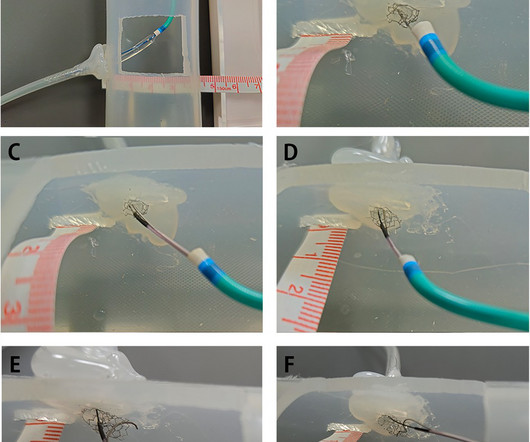
BackgroundPercutaneous coronary intervention (PCI) through the aorto-ostial coronary stent that is protruding into the aorta remains a technical challenge because of the poor coaxial alignment of the guiding catheter and the inability to advance the guidewire into the distal vessel through the stent's central lumen.
We included major adverse cardiovascular events (MACE), myocardialinfarction (MI), cardiac death and other outcome indicators. ConclusionsCompared with the non-IVUS-guided group, IVUS-guided stent implantation may be more effective for patients with complex CAD.Systematic Review RegistrationPROSPERO [CRD42024531366].
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content