This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
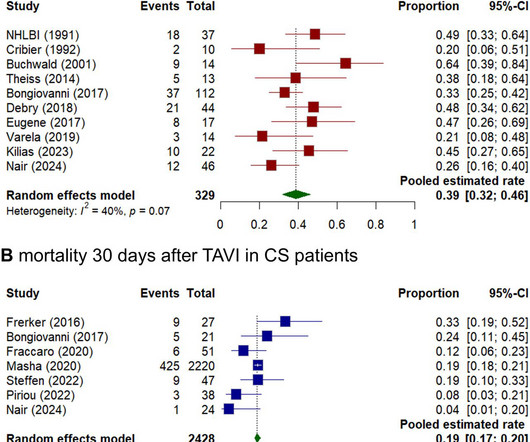
Background Cardiogenic shock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. Despite advancements in emergency interventions, the optimal treatment approach remains uncertain. Methods A systematic literature review and meta-analysis was performed. The primary endpoint was mortality at 30 days.
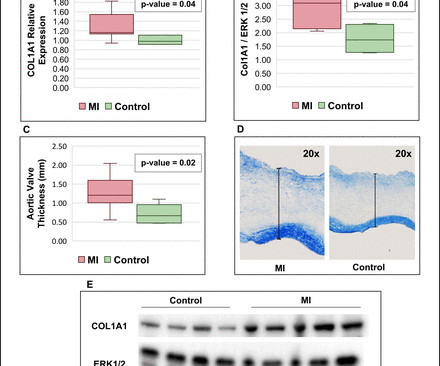
Background Myocardialinfarction (MI) has been shown to induce fibrotic remodelling of the mitral and tricuspid valves. It is unknown whether MI also induces pathological remodelling of the aortic valve and alters aortic stenosis (AS) progression.
Despite this, the patient went on to develop chest pain, which was accompanied by electrocardiographic signs of acute extensive anterior wall myocardialinfarction and elevated troponin I levels.
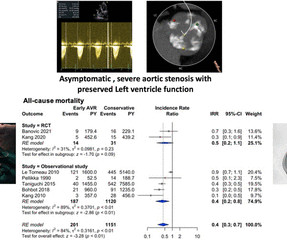
Background A quarter of patients with severe aortic stenosis (AS) were asymptomatic, and only a third of them survived at the end of 4 years. Only a select subset of these patients was recommended for aortic valve replacement (AVR) by the current American College of Cardiology/American Heart Association guidelines.
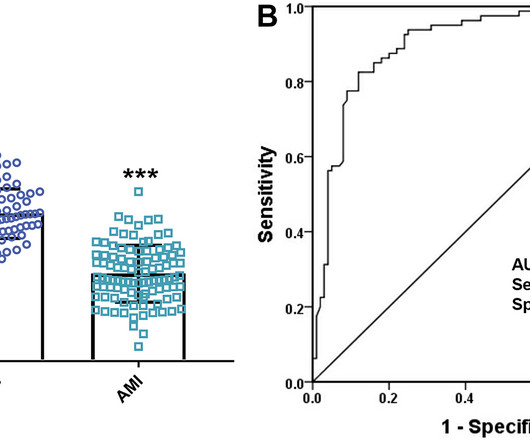
The purpose of this study was to explore the expression of miR-665 in acute myocardialinfarction (AMI) and evaluate its significance in the diagnosis and prognosis of AMI.
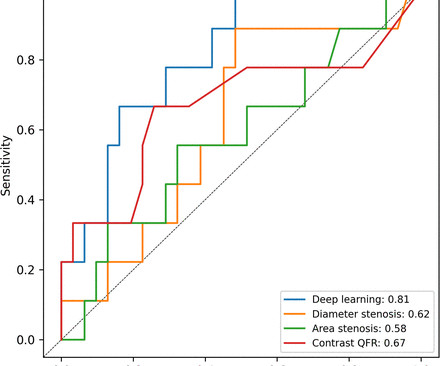
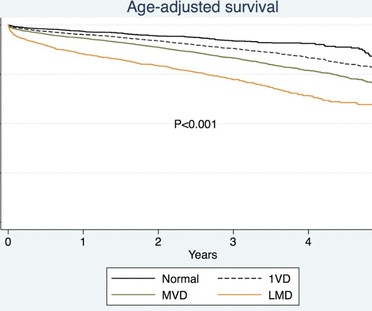
Background Angiographic parameters can facilitate the risk stratification of coronary lesions but remain insufficient in the prediction of future myocardialinfarction (MI). Among all models, DL demonstrated the highest accuracy (0.78) followed by QFR (0.70) and area stenosis (0.68).
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The angiographer uses a denominator that is too small, thereby underestimating the degree of stenosis.
We performed coronary angiography for the patient with ECMO support, indicating that the patient had an 80% critical stenosis of the left main coronary artery and an 80%–90% stenosis in the middle section of the left anterior descending artery with an aneurysm. Fortunately, there was no obvious stenosis in the right coronary artery.
Such a pattern is consistent with significant left main coronary artery stenosis. Angiography done after initial stabilization showed severe stenosis of distal left main coronary artery. ST segment elevation is noted in aVR. Clinical evaluation and X-Ray chest showed features of pulmonary edema. J Am Coll Cardiol. Engelen DJ et al.
Comparison Summary: ANTEROLATERAL ST CHANGES ARE NOW MORE PRONOUNCED, RATE DEPENDENT VS ISCHEMIC CHANGES Here is the Queen's diagnosis: The cath lab was activated: Culprit Lesion (s): Thrombotic 99% mid LAD stenosis with TIMI II flow Peak troponin not measured, unfortunately. So we don't have a good idea how large the final infarct size was.
The NOTION trial, a pioneering study, sought to compare the long-term clinical and bioprosthesis outcomes of Transcatheter Aortic Valve Implantation (TAVI) versus Surgical Aortic Valve Replacement (SAVR) in patients with severe aortic valve stenosis (AS) at lower surgical risk.
Advances in cardiovascular imaging have improved the ability to identify coronary artery stenosis in patients with KD, yet knowledge gaps remain regarding optimal frequency of serial imaging and the best imaging modality to identify those at risk for inducible myocardial ischemia.
BackgroundLp(a) (lipoprotein(a)) is an independent risk factor for calcific aortic valve stenosis (CAVS). Journal of the American Heart Association, Ahead of Print. Whether patients with CAVS and high Lp(a) levels are at higher risk of valvular or cardiovascular events is unknown. The maximal followup time was set to 5 years.
Smith: This is an enormous myocardialinfarction. The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1. Diagnosis of Occlusion MyocardialInfarction in Patients with Left Bundle Branch Block and Paced Rhythms. Next trop in AM. ng/mL - 80.0
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chest pain patients.
Among the patients included, those with diabetes exhibited higher rates of adverse events, including death, spontaneous myocardialinfarction (MI), and repeat revascularization. Patients were stratified based on diabetes status, and various outcome measures were assessed using Kaplan-Meier event rates and Cox model hazard ratios.
mg tablet), ananti-inflammatory atheroprotective cardiovascular treatment, to reduce the risk of myocardialinfarction (MI), stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple risk factors for cardiovascular disease.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
Objective The optimal medical therapy after surgical aortic valve replacement (SAVR) for aortic stenosis remains unknown. Methods All patients undergoing SAVR due to aortic stenosis in Sweden 2006–2020 and surviving 6 months after surgery were included.
Background Untreated multivessel disease (MVD) in acute myocardialinfarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year.
Coronary angiography gives a visual impression about the severity of the stenosis. But it need not imply the actual functional significance of the stenosis in terms of flow physiology. They had lower rates of mortality or myocardialinfarction. myocardialinfarction rate and 3.2% Normal FFR is 1.0
The timely detection of myocardial fibrosis is crucial for intervention and improved outcomes. 68 Ga-FAPI-04 PET/CT shows promise in assessing fibroblast activation in patients with early myocardialinfarction characterized by prolonged myocardial ischemia.
Coronary computed tomography angiography (CTA) showed diffuse stenosis in the left anterior descending and the first diagonal branch arteries. We reviewed English case reports of cardiac cephalalgia from 1982 to 2022 using PubMed ([link] Results A 69-year-old man presented with a sudden headache without triggers or typical symptoms.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. There may be a chronic tight stenosis and a non-obstructed lesion that thrombosed.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Results Clinical outcomes including mortality at 30 days, perioperative myocardialinfarction, number of grafts, incidence of stroke, rate of further need for revascularisation, and patient-reported quality of life did not differ in CABG guided by functional testing from those guided by traditional angiography.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardialinfarction (type II) and acute coronary stent thrombosis (type III). Emergency coronary angiography showed coronary spasm and moderate lumen stenosis in the middle segment of left anterior descending artery (LAD).
The incidence of the primary endpoint (death, MI, or repeat revascularization) was compared between FFR- and angiography-guided PCI according to non-IRA stenosis severity (QCA stenosis ≥70% or <70%).Results:A There was no significant interaction between treatment strategy and non-IRA stenosis severity (p for interaction=0.636).
What do you think the prehospital ECG showed (with pain)? __ Cardiology: culprits for the patient's non-ST elevation myocardialinfarction and syncopal event with possible arrhythmic etiology include occlusion of the distal LAD (chronicity uncertain) and severe stenosis of the proximal first diagonal branch.
Objective:To compare the 1-month stroke, myocardialinfarction (MI), and/or death rates among symptomatic patients undergoing either CAS or CEA according to the timing of the procedure in Carotid Revascularization Endarterectomy versus Stenting Trial (CREST).Methods:We
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes et al. Eur Heart J 2018.
Diagnosis of Acute MyocardialInfarction in the Presence of Left Bundle Branch Block using the ST Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. Electrocardiographic Diagnosis of Acute Coronary Occlusion MyocardialInfarction in Ventricular Paced Rhythm Using the Modified Sgarbossa Criteria.
The primary outcomes included a 30-day stroke or transient ischemic attack, myocardialinfarction, and mortality. Furthermore, subgroup analyses were performed based on age and degree of stenosis. 1.82]) and myocardialinfarction (OR, 1.29 [95% CI, 0.83–2.01]) 2.01]) but lower mortality (OR, 0.42 [95% CI, 0.22–0.81]).
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardial ischemia, but no clear stenosis of coronary artery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024.
Coronary computed tomography angiography (CCTA) is routinely used to diagnose CAD caused by the narrowing (stenosis) or blockage of the coronary arteries that supply the heart with blood. More than 8 million Americans visit hospital emergency departments experiencing chest pain every year. In June 2023, the U.S.
Objective Coronary angiography (CA) and percutaneous coronary intervention (PCI) is of great importance during non-ST-segment elevation myocardialinfarction (NSTEMI) management. Conclusion Coronary lesions (>50% stenosis) are strong predictors of mortality in elderly patients with NSTEMI. –7.6) and HR 4.5 (1.6–12.5).
Patients with diabetes experienced higher rates of 5-year death (158/1104 [Kaplan-Meier rate, 14.7%] versus 297/3289 [9.3%];P<0.001), spontaneous myocardialinfarction (MI; 67/1104 [6.7%] versus 114/3289 [3.7%];P<0.001), and repeat revascularization (189/1104 [18.5%] versus 410/3289 [13.2%];P<0.001).
Abstract: Transcatheter aortic valve replacement (TAVR) is an interventional procedure performed in patients with severe aortic stenosis and often required perioperative antiplatelet therapy. There were no significant differences in the incidence of other bleeding events, transfusions, stroke, myocardialinfarction, or all-cause death.
In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. Am Heart J (1989) 117 : pp 657-665. de Zwaan C.,
Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP? Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102). The ST depressions in I and aVL have resolved. Murakami MM.
BACKGROUNDCarotid artery stenting (CAS) has emerged as a viable alternative to carotid endarterectomy for managing carotid artery stenosis in high‐risk patients. Outcomes of interest were stroke, transient ischemic attack, death, myocardialinfarction, and access site complications. 1.96]; I2= 0%). 1.98]; I2= 0%).CONCLUSIONNo
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content