This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
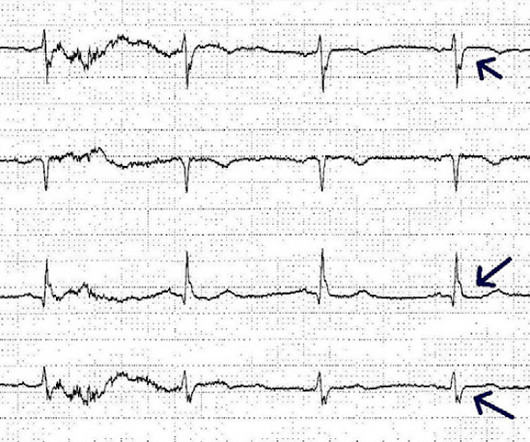
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Smith: This is an enormous myocardialinfarction. Most large STEMI have peak troponin I in the 20.0
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). We present the case of a man in his 50s, admitted with cardiac arrest secondary to inferolateral STEMI.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
Subtle as a STEMI." (i.e., She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen. 2012;1:344–348.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
He underwent coronary stenting (uncertain which artery). He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. I do not have the post-resuscitation ECG. He underwent months of rehabilitation and was able to return to work part time. Could this have been avoided?
Nature Reviews Cardiology, Published online: 02 April 2024; doi:10.1038/s41569-024-01020-2 In ST-segment elevation myocardialinfarction, the role of interventional modification of thrombi in the coronary arteries before stenting is controversial.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty.
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH? The criteria of Armstrong et al. References 1.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102). Murakami MM.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
There is an obvious inferior posterior STEMI(+) OMI. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E.
The near-immediate or instant feedback learning process by which the heart responds to any new invasive procedural variation facilitates each new change; be it drug-eluting stent, drug-coated balloon, or both in different combinations and permutations.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L. 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later.
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. He was found to have a 100% circumflex lesion for which a bare metal stent was placed.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction.
One of our fine interns, Daniel Lee, who is also an ECG whiz, found this paper from 2013 and brought it to my attention: The delayed activation wave in non-ST-elevation myocardialinfarction. When present, the infarct artery is more likely to be the circumflex. Of all inferior STEMI, 85% are due to RCA.
Because of the high troponin, echocardiography was done and showed a wall motion abnormality in the anterior, anterolateral, and apical walls, consistent with LAD myocardialinfarction. It was stented. The possibility of anterior STEMI was not noticed during patient care.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. A New ST-segment elevation myocardialinfarction equivalent pattern? An Impella was placed for cardiac output augmentation.
The ECG is diagnostic of occlusion myocardialinfarction (OMI). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The overall read is OMI with HIGH confidence. == Below is the ECG of Patient #2 — as interpreted by the QOH.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. This confirms these Q waves are caused by an acute infarct. But the ECG still doesn’t meet STEMI criteria. Smith : Normal ST Elevation in V2-V4 never has an associated Q-wave! the computer interpretation 2.
A very large myocardialinfarction. The next day the ECG not unexpectedly shows a completed transmural inferior and posterior wall infarction. The patient, albeit very delayed was referred for angiography where a 99% stenosed pRCA was stented. No further episodes of atrial fibrillation occurred during monitoring.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor.
ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. The "criteria" for posterior STEMI are 0.5 Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis? Is it STEMI or NonSTEMI? The troponin I returned at 4.1 mm STE in one lead. There is zero ST Elevation. This includes: 1.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
Angiogram: Culprit for the patient's inferior ECG changes and non-ST elevation myocardialinfarction is a 100% acute thrombotic occlusion of the proximal RCA. It was opened and stented. The patient was diagnosed with a"Non-STEMI." They have large infarcts and high mortality. To me, that is a meaningless diagnosis.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? Am Heart J.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. NTG drip started. Is this OMI?
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement. As the conversation progressed, another ECG spontaneously printed. The pathology is now painfully evident.
The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. Considerations on the naming of myocardialinfarctions. J Electrocardiol.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. A mid-LAD culprit lesion was identified and stented. Smith comment : V5 and V6 are excessively discordant!!!! Pacing Clin Electrophysiol.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. But which myocardial walls are affected? He did, found the true culprit, and went back in to stent it. This prehospital ECG was recorded: Here are limb leads: Here are precordial leads: Diagnosis? Can you tell from this ECG?
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. A 99% LAD occlusion was stented. Attached is the first ECG.
It is equivalent to a transient STEMI. This is diagnostic of myocardialinfarction. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? 100% LAD occlusion.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content