This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Introduction ST-elevation myocardialinfarction (STEMI) is one of the most prevalent presentations in young patients. Methods A retrospective, multicentre cohort study was carried out in 6799 patients diagnosed with STEMI. to 1.54) (p<0.042).
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardialinfarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
ST-elevation myocardialinfarction (STEMI) is a critical cardiovascular emergency characterized by acute coronary artery occlusion and subsequent myocardial injury. The current standard of care is primary percutaneous coronary intervention (PPCI), which aims to rapidly restore epicardial blood flow.
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardialinfarction (STEMI).MethodsA
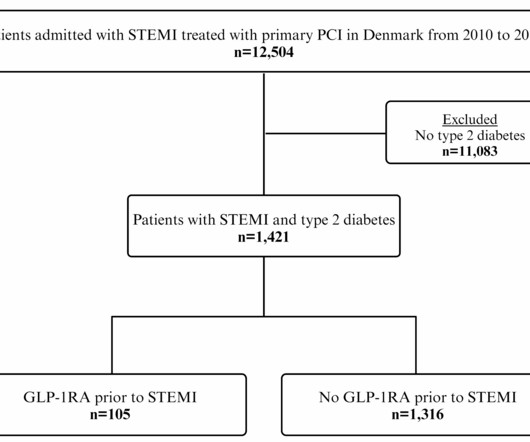
Yet, the impact of GLP-1RA treatment before ST-segment elevation myocardialinfarction (STEMI) on. Glucagon-like peptide-1 receptor agonist (GLP-1RA) treatment reduces cardiovascular events in type 2 diabetes.
This randomized clinical trial investigates if prehospital pulse-dose glucocorticoid treatment has a cardioprotective effect in patients with ST-segment elevation myocardialinfarction (STEMI).
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
The goal of the CLEAR SYNERGY OASIS 9 trial was to determine the long-term cardiovascular (CV) effects of colchicine following percutaneous coronary intervention (PCI) for ST-segment elevation or large non–ST-segment elevation myocardialinfarction (STEMI or NSTEMI, respectively).
Background The diagnosis of a left ventricular (LV) thrombus in patients with ST-segment elevation myocardialinfarction (STEMI) remains challenging. Methods We retrospectively evaluated 337 consecutive STEMI patients. The sensitivity for thrombus formation of the first and second TTE was 5.9% and 59%, respectively.
What is the impact of complete revascularization versus culprit-only revascularization on outcomes in older patients with ST-segment elevation myocardialinfarction (STEMI) and non–ST-segment elevation myocardialinfarction (NSTEMI)?
Background Different ST-segment elevation myocardialinfarction (STEMI) localizations go along with dissimilarities in the size of the affected myocardium, the causing coronary vessel occlusion, and the right ventricular participation. No significant associations of the STEMI localization with long-term mortality were found.
The goal of the CLEAR SYNERGY (OASIS 9) spironolactone trial was to determine the potential cardiovascular (CV) benefit of spironolactone following percutaneous coronary intervention (PCI) for ST-segment or large non–ST-segment elevation myocardialinfarction (STEMI or NSTEMI, respectively) regardless of post-MI left ventricular ejection fraction (..)
The MULTISTARS AMI (MULTivessel Immediate versus STAged RevaScularization in Acute MyocardialInfarction) trial compared immediate versus delayed percutaneous coronary intervention (PCI) of nonculprit lesions in patients with ST-segment elevation myocardialinfarction (STEMI) who underwent successful primary PCI of the culprit lesion.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
(MedPage Today) -- The heparin frequently given before percutaneous coronary intervention (PCI) should be pushed to as early as possible in patients with ST-segment elevation myocardialinfarction (STEMI), according to findings from the Chinese.
What are long-term clinical benefits of complete versus culprit-only revascularization among ST-segment elevation myocardialinfarction (STEMI) patients aged ≥75 years?
What is the safety and effectiveness of P2Y12 inhibitor pretreatment in patients transferred for primary percutaneous coronary intervention (PPCI) within a regional ST-segment elevation myocardialinfarction (STEMI) network?
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Opiates are associated with worse outcomes in MyocardialInfarction. Abstract 556.
Introduction Differences in pathophysiology, clinical presentation, and natural course of ST-elevation myocardialinfarction in female patients due to either spontaneous dissection (SCAD-STEMI) or atherothrombotic occlusion (type 1 STEMI) have been discussed. vs. 1.8 ± 5.1%, p = 0.002). vs. 1.8 ± 5.1%, p = 0.002).
Introduction ST-segment elevation myocardialinfarction (STEMI) diagnosis is based on a clinical presentation and ST-segment elevation (STE) in at least two consecutive leads. 1 This paradox stems from the incorporation bias and feedback sanction bias detailed in subsequent paragraphs.
What are the outcomes of bivalirudin vs. heparin anticoagulation during percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardialinfarction (STEMI)?
Percutaneous coronary intervention (PCI) can effectively restore myocardial perfusion in patients with ST-segment elevation myocardialinfarction (STEMI). Nevertheless, STEMI patients may still experience a n.
STEMI – Anterior Wall ECG shows ST elevation myocardialinfarction of anterior wall. Up sloping elevation of ST segment is seen in leads V1 to V5, with maximum ST elevation in V2, as is characteristic of anterior wall infarction. QS complexes are seen from V1 to V3.
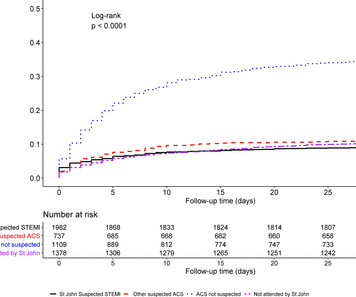
Background Early recognition of ST-segment elevation myocardialinfarction (STEMI) is needed for timely cardiac monitoring and reperfusion therapy. Results Of 5465 patients with STEMI, 73% were transported to hospital by ambulance. and non-ACS diagnosis in 29.7%.
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients.
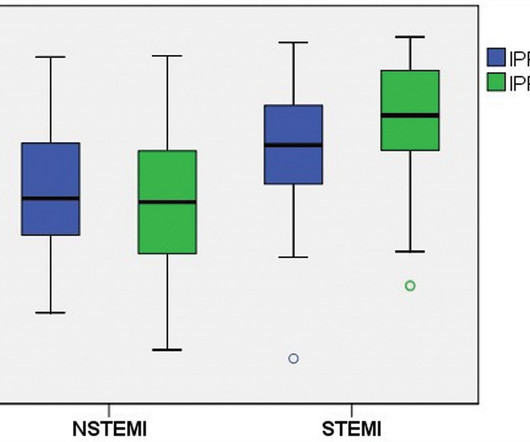
Introduction Elevated peak cardiac troponin levels have been linked with increased morbidity and mortality in patients with acute myocardialinfarction (AMI). Results Among the 277 patients diagnosed with AMI who underwent IPF testing, 113 had (STEMI) and 164 had (NSTEMI). Notably, among STEMI patients, those with IPF ≥ 4.2%
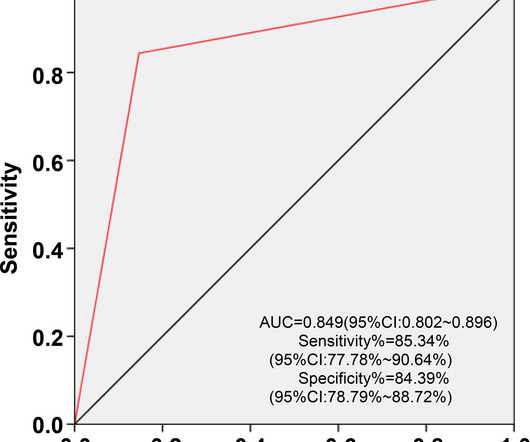
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardialinfarction (STEMI). Early recognition of HLI and accurate assessment of Killip classification is warranted for effective management of STEMI.
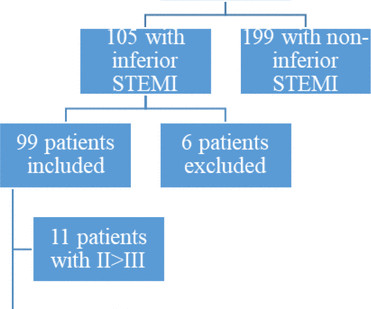
Background ST elevation myocardialinfarction (STEMI) represents a cardiac emergency. Inferior STEMI represents a dilemma for cardiologists. Methods We performed a single-centre retrospective cohort analysis of all patients admitted to our hospital from 2008 to 2020 with a diagnosis of inferior STEMI.
Background Despite restoration of epicardial blood flow in acute ST-elevation myocardialinfarction (STEMI), inadequate microcirculatory perfusion is common and portends a poor prognosis. Methods Comprehensive literature search of six electronic databases identified relevant randomised controlled trials.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
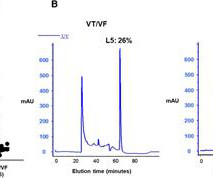
Background Early ventricular tachycardia/fibrillation (VT/VF) in patients with ST-elevation myocardialinfarction (STEMI) has higher morbidity and mortality. This study examines gender-differentiated risk factors and underlying mechanisms for early onset VT/VF in STEMI. vs. 61.0 ± 13.0 vs. 1.70 ± 0.28, P = 0.02
What is the impact of the administration of cangrelor at reperfusion on myocardialinfarct (MI) size and microvascular obstruction (MVO) in patients with ST-segment elevation myocardialinfarction (STEMI) undergoing primary percutaneous coronary intervention (PPCI)?
Objectives This study aimed to perform a meta-analysis of the short-term impact of ischaemic postconditioning (IPoC) on myocardial injury in ST elevation myocardialinfarction (STEMI) using surrogate cardiac biomarkers. These results resonate with some studies using imaging techniques to ascertain myocardial damage.
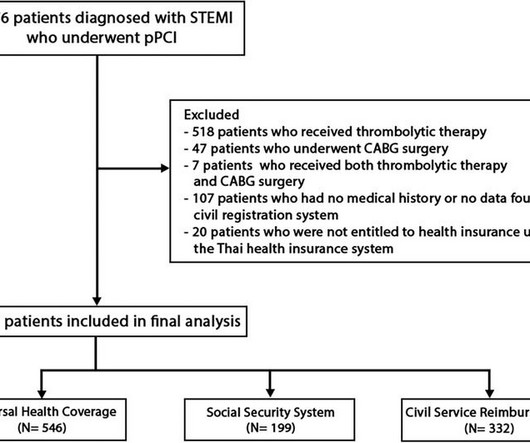
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardialinfarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
The benefits of complete revascularization over culprit-only coronary artery revascularization were confirmed in older patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel disease over the first 4 years, according to late-breaking research presented in a Hot Line session today at ESC Congress 2024.
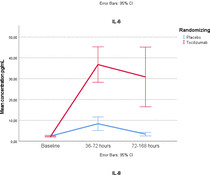
Background Tocilizumab improves myocardial salvage index (MSI) in patients with ST-elevation myocardialinfarction (STEMI), but its mechanisms of action are unclear. Methods STEMI patients were randomised to receive a single dose of 280 mg tocilizumab (n=101) or placebo (n=98) before percutaneous coronary intervention.
BackgroundCurrent research suggests that microvascular obstruction (MVO) following the first percutaneous coronary intervention (PCI) in myocardialinfarction patients is closely related to inflammatory responses. The predictive model incorporating LCR enhances the ability to predict MVO occurrence in patients with STEMI post-PCI.
However, its prognostic role following percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI) remains unclear. Echocardiography was performed upon admission and at 6 months post-myocardialinfarction (MI). vs. 6.231.91, P 8.13
Stress hyperglycemia ratio (SHR), associated with adverse outcomes in patients with ST-segment elevation myocardialinfarction (STEMI), has several definitions. This study aims to assess the prognostic value o.
The goal of the HELP-PCI trial was to determine the efficacy and safety of administering unfractionated heparin at first medical contact versus during cardiac catheterization only in patients with ST-segment elevation myocardialinfarction (STEMI).
Introduction Cardiogenic shock (CS) complicates 5%–15% of cases of acute myocardialinfarction (AMI) with inpatient mortality greater than 40%. This prospective registry includes all patients >18 years of age presenting with STEMI with or without CS beginning on 1 February 2023.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content