

Differences in left ventricular myocardial function and infarct size in female patients with ST elevation myocardial infarction and spontaneous coronary artery dissection
Frontiers in Cardiovascular Medicine
JANUARY 7, 2024
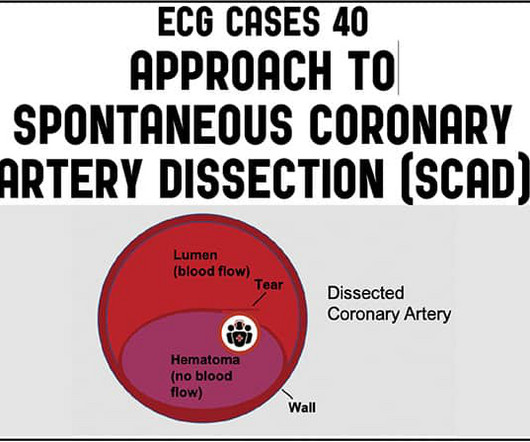
Introduction Differences in pathophysiology, clinical presentation, and natural course of ST-elevation myocardial infarction in female patients due to either spontaneous dissection (SCAD-STEMI) or atherothrombotic occlusion (type 1 STEMI) have been discussed. vs. 1.8 ± 5.1%, p = 0.002).












Let's personalize your content