This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Introduction Differences in pathophysiology, clinical presentation, and natural course of ST-elevation myocardialinfarction in female patients due to either spontaneous dissection (SCAD-STEMI) or atherothrombotic occlusion (type 1 STEMI) have been discussed. vs. 1.8 ± 5.1%, p = 0.002). vs. 1.8 ± 5.1%, p = 0.002).
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.
BackgroundSpontaneous coronary artery dissection (SCAD) significantly contributes to myocardialinfarction among young individuals. After excluding single nucleotide polymorphisms (SNPs) confounded by extrinsic variables, the association of neuroticism scores with SCAD susceptibility persisted.
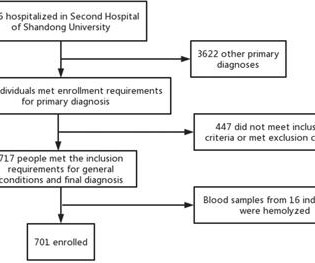
Background To investigate the correlation between lg (circSCMH1/miR-874) and acute coronary syndrome (ACS), acute myocardialinfarction (AMI), and carotid plaque stability. Methods 701 patients were divided into stable coronary artery disease (SCAD), ACS, and control groups.
In the absence of these factors it is termed spontaneous coronary artery dissection ( SCAD ). At that time the literature suggested: SCAD was rare , Mostly related to pregnancy , Seen on angiography as a dissection flap , and Managed similarly to MI caused by CAD (ASA, BB, lytics/PCI ). The SCAD cases in Lobo et al. Lobo et al.
This is diagnostic of myocardialinfarction. What is Spontaneous Coronary Artery Dissection (SCAD)? I asked Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital (and Minneapolis Heart Institute) and an aspiring cardiologist, to write a couple paragraphs on SCAD.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. Currently, SCAD is a diagnosis that can only be established emergently in the cath lab with angiography. Lupu L, Taha L, Banai A, et al. And is there new left bundle branch block (LBBB)?
MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). Spontaneous coronary artery dissection (SCAD) should be considered as a cause of MINOCA. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. What is MINOCA?
Spontaneous coronary artery dissection (SCAD) is an uncommon condition which is increasingly recognized as a cause of significant morbidity. SCAD can cause acute coronary syndrome and myocardialinfarction (MI), as well as sudden cardiac death. The standard of care for patients with SCAD is rapidly evolving.
Background Contemporary management of spontaneous coronary artery dissection (SCAD) is still controversial. Results The systematic review included 13 observational studies evaluating 1,801 patients with SCAD. Results The systematic review included 13 observational studies evaluating 1,801 patients with SCAD. Approximately 48.5%
Background Spontaneous coronary artery dissection (SCAD) and Takotsubo syndrome (TTS) constitute two common causes of nonatherosclerotic acute cardiac syndrome particularly frequent in women. Results A total of 289 SCAD and 150 TTS patients were included; 89% were women. In-hospital events (43.3% vs. 7.1%, HR 5.3, vs. 9.6%, HR 4.5,
MINOCA now encompasses Spontaneous Coronary Artery Dissection (SCAD), a rare condition that is known to manifest primarily in women and affects the epicardial coronary artery. Despite padding the MINOCA numbers with SCAD, MINOCA is much rarer than conventional epicardial coronary disease. Which is exactly what the numbers show.
It was not SCAD (coronary dissection) Highest troponin I was 37,000 ng/L, but it was not measured to peak. Acute type A aortic dissection presenting as ST-segment elevation myocardialinfarction referred for primary percutaneous coronary intervention. This was ruptured plaque with thrombus. Some Literature 1.3% Acta Cardiol.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content