This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
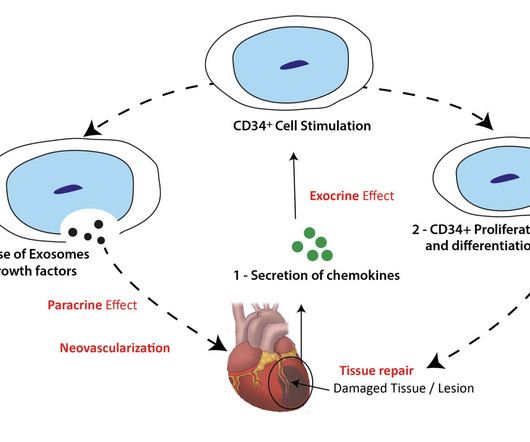
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, announced success from a collaborative Phase II trial of ProtheraCytes for the treatment of acute myocardialinfarction (AMI) led by CellProthera , as well as plans to continue the relationship into Phase III.
Specific cardiovascular diseases, such as acute myocardialinfarction, arrhythmias, pulmonary hypertension and pericarditis, were also pointed. SiO2 exposure was linked to an increased risk of myocardialinfarction, with potential mechanisms involving inflammation and platelet activation.
A number of therapies that have been shown to be effective in patients with chronic heart failure, including beta-blockers, mineralocorticoid receptor antagonists, and renin–angiotensin system inhibitors, have also been shown to be beneficial in patients with evidence of left ventricular systolic dysfunction, pulmonary congestion, or both after an (..)
Pulmonary embolism is the most common cardiovascular disease after myocardialinfarction and stroke. Konstantinides (Eur Heart J 41(4):543–603, 2020) Current guidelines categorize patients with PE as being at.
Myocardialinfarction (MI) and pulmonary artery hypertension (PAH) are two prevalent cardiovascular diseases. This study aims to evaluate the effect of PTE on oxidative stress in the hearts of animals with myocardialinfarction and in the lungs of animals with PAH. Male Wistar rats were used in both models.
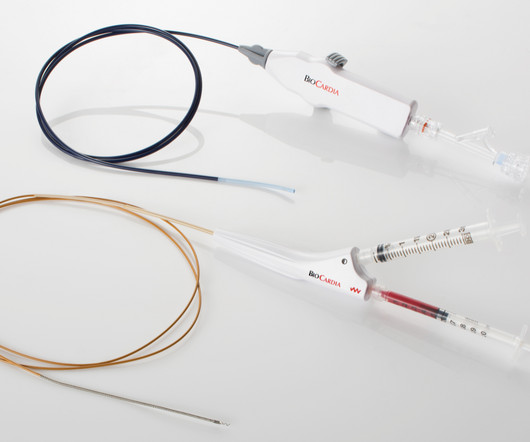
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, reported it has submitted a 510(k) for approval of its patented Morph DNA Steerable Introducer Sheath. mtaschetta-millane Wed, 07/31/2024 - 07:00 July 31, 2024 — BioCardia, Inc. ,
Figure 1 shows the chest radiograph of the first patient diagnosed with amiodarone pulmonary toxicity back in 1978.1 Amiodarone had been in use for the treatment of cardiac arrhythmias for more than a decade by the time we first identified a potential association of amiodarone therapy and pulmonary toxicity.1
a company focused on cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases announced that the Unites States Patent Office has granted Patent No: 12,036,371 titled “Method of Accessing the Left Atrium with a Multi-Directional Steerable Catheter,” with a patent term that will expire in 2035.
To me, this looks like pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. Angiogram: "ACS - Non ST Elevation MyocardialInfarction. This is a HUGE myocardialinfarction. Here are a few clips.
The primary outcome was risk of an ASCVD hospitalization composite outcome (myocardialinfarction, coronary artery bypass graft, percutaneous coronary intervention, stroke, transient ischemic accident) after COPD hospitalization relative to before COPD hospitalization. Journal of the American Heart Association, Ahead of Print.
COVID-19 likely increases relative risk (RR (95% CI)) of myocardialinfarction (3.3 (1.0 to 10)), pulmonary embolism (24.6 Other RTIs also likely increase the RR of myocardialinfarction (2.9 (95% to 11.0)), stroke (3.5 (1.2 to 44.9)) and deep venous thrombosis (7.8 (4.3 95% CI 1.8 to 4.9)) and stroke (2.6 (95%
The pooled risks for overall response rate (ORR), 1-year progression-free survival (PFS), adverse events (AEs), immune-related AEs, (irAEs), hypertension, and vascular events defined as stroke, myocardialinfarction and pulmonary embolisms, were calculated.
A pulmonary ultrasound was performed on admission and was considered positive (PE+) when there were three or more B-lines in two quadrants or more of each hemithorax. Methods We analyzed a cohort of patients admitted for ACS between February 2017 and February 2018. Results A total of 119 patients were included: 54.6% with ST elevation and 45.4%
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. The estimated pulmonary artery systolic pressure is 27 mmHg + RA pressure. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
Metadata was retrieved and transferred to bibliographic visualization software, VOSviewer, for co‐authorship and co‐occurrence analyses to identify trends in tenecteplase research.ResultsData visualization software identified three tenecteplase research clusters – myocardialinfarction, pulmonary embolism, and acute ischemic stroke.
Xray was consistent with pulmonary vascular congestion. Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L. Lung exam showed diffuse B lines bilaterally. 40 mg of furosemide was given.
male, 67% acute myocardialinfarction, 33% acute decompensated heart failure), 45 (41.3%), 33 (30.3%), and 31 (28.4%) were in SCAI Shock Stages C, D, and E, respectively. Patients achieving all 3 best practices significantly increased from 35.1% (P1) to 52.8% (P3) (P=0.026).
BackgroundCardiogenic shock complicating acute myocardialinfarction is associated with a high mortality rate. Cardiogenic shock after outofhospital cardiac arrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure. Of 789 patients included, 31.6%
Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardialinfarction (STEMI). Circulation, Volume 150, Issue Suppl_1 , Page A4142231-A4142231, November 12, 2024. The cut-off point was 14.9 ng/L, showing a < 4 or ≥ 4 TIMI score.
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio. J Cardiovasc Ultrasound. 2011 Dec;19(4):169-73.
We used previously validated ICD-10-CM codes for acute ischemic stroke, intracerebral and subarachnoid hemorrhage, cerebral venous thrombosis, acute myocardialinfarction, pulmonary embolism, and acute deep venous thrombosis to define our study outcome.Results:We identified a total of 747 patients with OHSS in HCUP.
Both of these patterns together suggest Aslanger's pattern , recently published in J Electrocardiology: A new electrocardiographic pattern indicating inferior myocardialinfarction. These suggest inferior OMI with possible RV involvement.
In SCAPE (sympathetic crashing acute pulmonary edema), Emergency providers seem now to regularly give high dose NTG, but when the BP is 170/105 in a patient who is not crashing, we often fail to give something to lower afterload. __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
Second , if the patient is hemodynamically stable, without pulmonary edema, it may be wise to try some fluids and and benzodiazepines and/or propofol for this post-seizure patient with likely high catecholamine levels. Place the Left Arm electrode on the 5th intercostal space, right sternal border. Monitor Lead I. de Lemos, J. Gibler, W.
Adverse vascular outcomes used as endpoints include acute ischemic stroke, acute myocardialinfarction, deep vein thrombosis/pulmonary embolism, AF, and carotid artery dissection.A Patients with any adverse vascular outcomes before the index ECG were excluded. The mean age at the time of the index ECG was 44.3
Smith, MD – Department of Emergency Medicine, Hennepin County Medical Center, Professor, University of Minnesota School of Medicine, Minneapolis, MN ABSTRACT: Background: Patients with type 1 myocardialinfarction with normal left ventricular function that are hemodynamically stable do not usually manifest with sinus tachycardia.
The ACC/AHA guidelines mandate less than 2 hours cath for patients with ACS with refractory pain, pulmonary edema, or electrical or hemodynamic instability. Unusual and puzzling, as there was a large focal acute MI) Final Diagnosis: Acute MI, Non ST Elevation MyocardialInfarction.
A subset of NSTEMI precipitated by acute severe HT and flash pulmonary edema has excellent prognosis if BP is reduced promptly. Anderson ML, Peterson ED, Peng SA, Differences in the profile, treatment, and prognosis of patients with cardiogenic shock by myocardialinfarction classification: A report from NCDR. J Clin Med.
Clinical evaluation and X-Ray chest showed features of pulmonary edema. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardialinfarction. ST segment elevation is noted in aVR. J Am Coll Cardiol. 2001 Nov 1;38(5):1348-54. Engelen DJ et al.
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardialinfarction (12.14% vs. 3.21%, (..)
Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis? The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We Patients with ACS and acute pulmonary edema 3.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. Her initial cTnI returned at 0.25 A CT Coronary angiogram was ordered.
MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). pulmonary embolism, sepsis, etc.), If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely. What is MINOCA?
The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. myocardialinfarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. Furthermore, a study compared patients with AS to patients without AS in acute pulmonary edema who received nitrates.
Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk. The computerized interpretation for this tracing was, “Sinus rhythm; Normal ECG” — and attention of acute care providers was apparently focused on attending to this patient’s pulmonary problems. Murakami M.
The VARIPULSE Platform is designed to enable pulmonary vein isolation with the versatility of a catheter loop, a simple generator user interface, and a mapping system that provides an intuitive, reproducible workflow with real-time visualization, contact indicator, and PF tagging mechanisms.
Sacubitril/valsartan and a mineralocorticoid receptor anatogonist (MRA) can be initiated safely and used simultaneously in post-myocardialinfarction complicated by left ventricular (LV) dysfunction, congestion or both – Insight from the PARADISE MI trial.
Covariates were adjusted for age (years), pulmonary congestion, percutaneous coronary intervention, left ventricular ejection fraction (%) and hypertension. The cohort comprised patients with AMI and pulmonary congestion and/or left ventricular ejection fraction 40%.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. Use of diuretics is strongly associated with hypokalemia and ventricular fibrillation in myocardialinfarction.
During the hospitalization, they had higher rates of renal failure, pulmonary artery catheter use, and mechanical circulatory support use. In-hospital mortality was lower in transferred patients39.1% versus 47.1%; unadjusted odds ratio (OR), 0.71 (95% CI, 0.700.73); adjusted OR, 0.73 ([95% CI, 0.710.76];P<0.001).
Introduction:Cardio-cerebral infarction, a rare clinical presentation involving simultaneous acute ischemic stroke and acute myocardialinfarction, poses significant therapeutic challenges. The incidence of this dual infarction is currently unknown due to its rarity. An open-heart surgery was considered.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content