This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Heart failure with preservedejectionfraction is a recognised outcome in patients with myocardialinfarction, although heart failure with reduced ejectionfraction is more common. Among patients with myocardialinfarction, a 1-SD increase in pulse pressure was associated with a 1.60-fold
Heart failure (HF) is one of the significant complications in patients with myocardialinfarction (MI), leading to increased risk for cardiovascular morbidity and mortality. 2 However, mortality rate is greater in HF cases developing >3 days following MI compared with less than or equal to 3 days after MI.
Beta-blockers are commonly used in patients with heart failure and mildly reduced or preservedejectionfraction (HFmrEF/HFpEF). Methods and results We pooled individual patient data from four large HFmrEF/HFpEF trials (I-Preserve, TOPCAT, PARAGON-HF, and DELIVER).
Abstract Aims Preventive strategies for heart failure (HF) with preservedejectionfraction (HFpEF) include pharmacotherapies and lifestyle modifications. All had no evidence of HF or myocardialinfarction prior to completion of the ETT. Thus, we evaluated the association between CRF and HFpEF incidence.
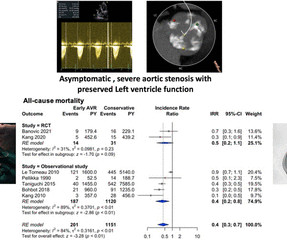
The secondary outcomes were composite major adverse cardiac events (MACE) (study defined), myocardialinfarction (MI), stroke, cardiac death, sudden death, the development of symptoms, heart failure hospitalisations and major bleeding. The primary outcome was all-cause mortality. PROSPERO registration number CRD42022306132.
BACKGROUND:Apparent treatment-resistant hypertension (aTRH) is prevalent and associated with adverse outcomes in heart failure with mildly reduced or preservedejectionfraction. Less is known about the potential role of sodium-glucose co-transporter 2 inhibition in this high-risk population. per 100 patient-years).
Spironolactone improved outcomes in patients with severely symptomatic HF with reduced ejectionfraction, and later, eplerenone expanded the benefits to patients with mildly symptomatic HF with reduced ejectionfraction and myocardialinfarction complicated by HF.
Patients diagnosed with reduced ejectionfraction (HFrEF) and with heart failure with mildly reduced ejectionfraction (HFmrEF) were treated with Vericiguat combined with “ARNI, BB, MRA, SGLT2i” therapy. vs. 43.1 ± 8.5%, P < 0.01), LVEDD (60.5 ± 8.1 vs. 58.2 ± 7.3 mm, mm, P < 0.01), NT-proBNP (4,567.8 ± 5,163.9
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). STEP-HFpEF DM 5 ( NCT04916470 ) explored the effects of semaglutide in obesity-related HF with preservedejectionfraction (HFpEF) and type 2 diabetes. in the medical therapy group.
4] More recently, at least at the epidemiologic level, the obesity paradox has been confirmed in both heart failure with reduced ejectionfraction (HFrEF) and heart failure with preservedejectionfraction (HFpEF), but also in those with coronary heart disease. [5, Carbone, Salvatore, et al. Future Cardiology 13.5
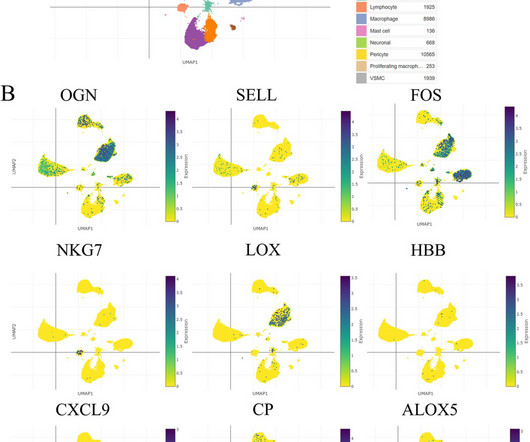
BackgroundThe mortality of patients with acute myocardialinfarction (MI) raised rapidly in last decade and obesity are becoming the major cause to CAD progression, thus inducing heart failure preservedejectionfraction (HFpEF). Also, SASPs decreased in hypoxic fibroblasts after OGN knockdown.
Emerging Risk Factors: Non-traditional factors such as the microbiome, pollution, and somatic mutations are increasingly linked to “SMuRFless” myocardialinfarction (MI) cases.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content