This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
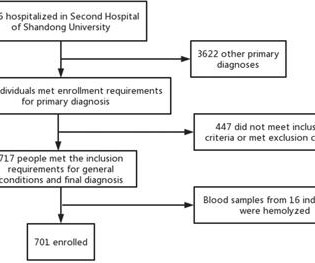
The goal of the PACMAN-AMI trial was to demonstrate the efficacy of early administration of alirocumab on plaque characteristics among patients undergoing percutaneous coronary intervention (PCI) for an acute myocardialinfarction (AMI).
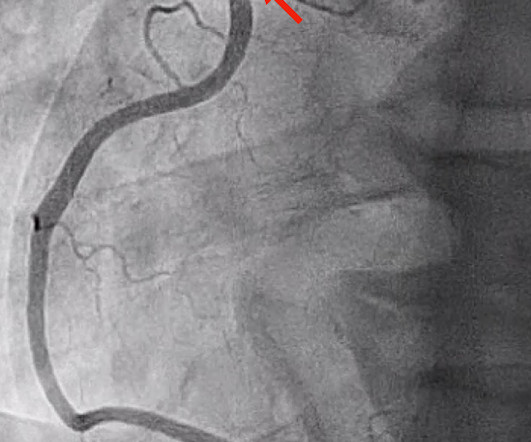
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. Fig 1 shows typical examples of two such plaques.
For life-threatening events involving complete occlusion of a coronary artery, the activation of ST-elevation myocardialinfarction protocols instructs the emergency services to provide immediate treatment and liaise directly with cardiac centres regarding invasive management, in turn, reducing morbidity and saving lives. 1 In this.
Background To investigate the correlation between lg (circSCMH1/miR-874) and acute coronary syndrome (ACS), acute myocardialinfarction (AMI), and carotid plaque stability. Compared with the low-risk plaque and control groups, the lg (circSCMH1/miR-874) value of medium-high risk plaque group decreased ( P < 0.05).
BackgroundProtruding aortic plaque is known to be associated with an increased risk for future cardiac and cerebrovascular events. Coronary plaque characteristics were compared to evaluate coronary plaque vulnerability in patients with protruding aortic plaque on computed tomography angiography.
Myocardialinfarction with non-obstructive coronary arteries (MINOCA) defines a heterogeneous group of atherosclerotic and non-atherosclerotic conditions, causing myocardial injury in the absence of obstructive coronary artery disease.
eGC shedding could contribute to atherosclerotic plaque vulnerability and acute myocardialinfarction (AMI) installation. The integrity of this structure sustains some vascular properties such as shear stress-induced nitric oxide release and the prevention of platelets and neutrophils adhesion on the vessel surface.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. MINOCA I do not have the bandwidth here to write a review of MINOCA.
We investigated whether treatment with LDE-paclitaxel changes plaque progression by coronary CT angiography and is safe in patients with chronic coronary artery disease. Among those, 58% had diabetes, 50% had myocardialinfarction, and 91% were in use of statin and aspirin.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardialinfarction (type II) and acute coronary stent thrombosis (type III). Here we share a case of Kounis syndrome type I caused by an allergy caused by a Cryptopteran bite.
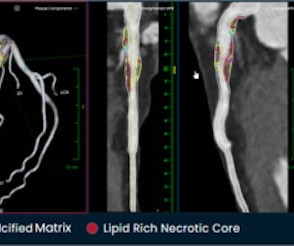
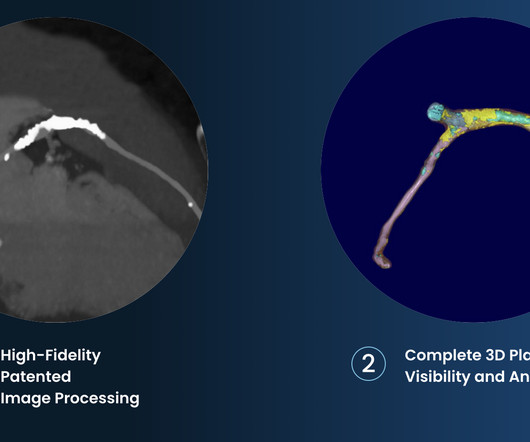
tim.hodson Tue, 10/01/2024 - 10:50 PHOTO CAPTION: The Elucid PlaqueIQ user interface is a fully interactive visualization of the patient’s coronary anatomy, showing specific plaque type and amount across various views to inform physician assessment of risk and patient-specific treatment pathway.
Elevated Lp(a) concentrations in patients with ischaemic heart disease have been linked to higher rates of peri-procedural myocardialinfarction (MI) during percutaneous coronary intervention (PCI). This review summarises the available data on the modulatory effect of Lp(a) on plaque morphology and recurrent ischaemic events.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) Although it is statistically unlikely, multiple plaque ruptures are possible. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. Heitner et al.
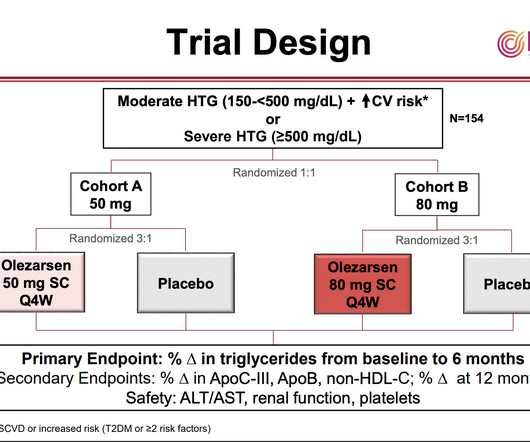
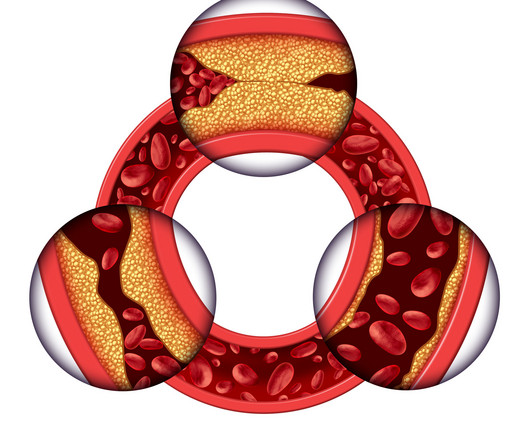
As with elevated LDL-cholesterol, high levels of triglycerides and the lipid particles on which they are carried in the blood can contribute to the formation of “plaques” in the arteries that impede blood flow and can lead to heart attacks and strokes. Triglycerides store unused calories and provide energy to the body.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? Murakami MM.
Background:The no-reflow has been reported to be associated with larger infarct size and mortality after acute myocardialinfarction (AMI). The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The vs. 8.6%, p < 0.001).
Plaque regression can be demonstrated by ultrasound evaluation of the carotids which are easily accessible. Maintaining normal blood pressure also reduces the risk of stroke and myocardialinfarction. Of course, exercise burns out extra calories and reduces body weight, which in turn is due to a decrease in the fat deposits.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). It can only be seen by IVUS. MINOCA has many etiologies. Learning Points: 1.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." FFR can be useful.
This article describes the pathway from gene discovery to novel therapeutic approaches that are now entering man.HDAC9expression is elevated in human atherosclerotic plaque, while in animal and cellular models, reducing HDAC9 (histone deacetylase 9) protein is associated with reduced disease.
She was diagnosed with NSTEMI with a thrombolysis in myocardialinfarction (TIMI) score of 5. Her EKG showed marked left-axis deviation, ST depressions in V2-V4, and RBBB. PCI, particularly with the Carlino technique, offers a reliable approach.
Permanent coronary ligation was performed to establish myocardialinfarction (MI). Compared with animals without PCOS, PCOS animals showed significantly exacerbated atherosclerotic plaque development and post-MI cardiac remodeling.
Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise. A New ST-segment elevation myocardialinfarction equivalent pattern? Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion MyocardialInfarctions.
Answer: This is MINOCA -- MyocardialInfarction with Non-Obstructive Coronary Arteries. Possible etiologies (depending on your definition) include: plaque rupture with spontaneous recanalization, coronary artery vasospasm, spontaneous coronary artery dissection, or other rarer causes. The name is self-explanatory.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. Because: 1) He has been reading this blog for a long time. 2) He is curious This is how Pendell got started.
Recent research has illuminated the role of total coronary atherosclerotic plaque activity across the entire coronary arterial tree in predicting patient-level clinical outcomes. Vessel-level coronary atherosclerotic plaque activity was assessed using coronary 18 F-sodium fluoride positron emission tomography (PET). 3.72; P = 0.013).
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He was switched from DAPT to aspirin and warfarin because he was considered a “DAPT failure.”
There are numerous other conditions leading to this kind of damage, which can trigger thrombus formation, causing strokes and myocardialinfarctions. The thrombogenic hypothesis, that endothelial damage and subsequent clot formation underlies the formation and growth of plaques, may represent a better model for ASCVD.
The term MINOCA stands for Myocardialinfarction with non-obstructive coronary arteries. She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e I’ll try and explain this a bit better by using a case study.
This is diagnostic of myocardialinfarction. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. She felt more comfortable being admitted. Int J Cardiol.
It was actually a dissection, not an atherosclerotic plaque rupture. Here it is: Obvious mid-RCA severe stenosis, but there is flow (reperfusion, spontaneous, autolysis) Female patient: She had a 2nd Obtuse Marginal occlusion (Left dominant, off the circumflex!). Reperfusion early and without T-wave inversion! Learning Points 1.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Here is the abstract: Background Identification of ST elevation myocardialinfarction (STEMI) is critical because early reperfusion can save myocardium and increase survival.
Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. Revascularization in Patients With Spontaneous Coronary Artery Dissection and ST-Segment Elevation MyocardialInfarction.
Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. I saw this result the next day and it perplexed me, so I inquired with the cardiologists. The proposed mechanism is complex.
Both of these patterns together suggest Aslanger's pattern , recently published in J Electrocardiology: A new electrocardiographic pattern indicating inferior myocardialinfarction. Angiogram Culprit Lesion: 90% mid LAD stenosis with evidence of plaque rupture, TIMI III flow on angiography.
The Hidden Threat: SMuRFless MyocardialInfarctions A concerning trend in CVD is the increase in myocardialinfarctions (MI) among individuals without standard modifiable risk factors (SMuRFless MI).
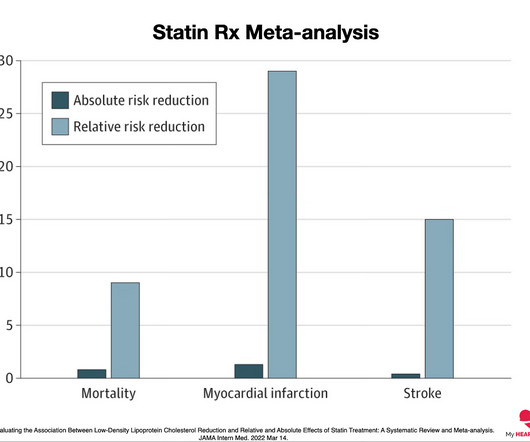
A heart attack is when that plaque ruptures and stops blood flow down the artery. This graph shows the absolute and relative risk reduction for statin therapy in preventing heart attacks (MyocardialInfarction), strokes and preventing death from any cause (All-cause mortality) 2. Cholesterol is an essential part of that process.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. LAD plaque with 0-25 percent stenosis. I do not have her previous ECGs, but reportedly these T-wave inversions were not present previously. Her initial cTnI returned at 0.25
mg tablet), ananti-inflammatory atheroprotective cardiovascular treatment, to reduce the risk of myocardialinfarction (MI), stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple risk factors for cardiovascular disease. mg on atherosclerotic plaque.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content