This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
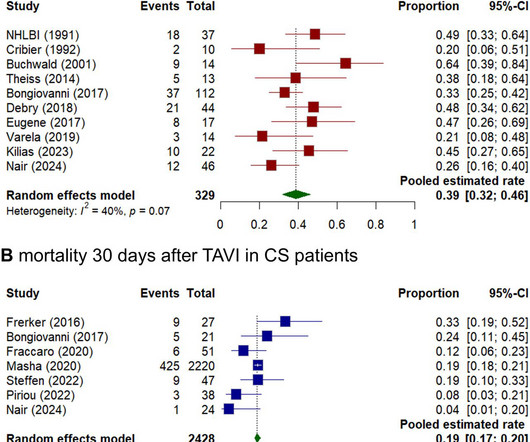
Secondary endpoints were in-hospital mortality, 1-year mortality, bleeding, major vascular complications, myocardialinfarction, stroke, incidence of pacemaker implantation, acute kidney injury and aortic regurgitation. The primary endpoint was mortality at 30 days.
The patient underwent a dual-chamber pacemaker implantation for complete AV block. Coronary angiography showed mild, non-obstructive atherosclerosis in the dominant left circumflex artery (LCx), which continued along the anatomical course of the RCA.
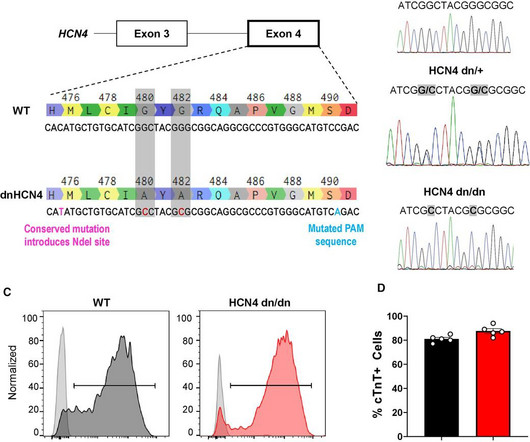
BackgroundHuman pluripotent stem cell-derived cardiomyocytes (hPSC-CMs) show tremendous promise for cardiac regeneration following myocardialinfarction (MI), but their transplantation gives rise to transient ventricular tachycardia (VT) in large-animal MI models, representing a major hurdle to translation.
I thought, it was pacemaker extrusion. It is an intentional exterior placement of a permanent pacemaker generator mimicking an extrusion due to pocket infection. Here is a patient, where a permanent pacemaker was kept temporarily for a few weeks or a month in high-risk reversible complete heart block situations.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Smith: This is an enormous myocardialinfarction. She reports associated SOB but no dizziness or LOC.
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. Hyperacute T Wave in the Early Diagnosis of Acute MyocardialInfarction. Interpretation of acute myocardialinfarction with persistent “hyperacute T waves” by cardiac magnetic resonance. She could not be resuscitated.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. She also has sick sinus syndrome (SSS) and intermittent high grade AV block for which she had a dual chamber pacemaker implanted.
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Usually does not exceed 160 bpm.
He has a pacemaker for an unknown arrhythmia reason, and has a hx of a PE but is not anti-coagulated currently. This is obviously diagnostic of inferior and lateral Occlusion MyocardialInfarction. The location of the infarct is clear, but that does not necessarily tell you what artery it is. It was central and constant.
He had previously undergone non‐contrasted head computed tomography (NCHCT) (magnetic resonance imaging (MRI) was unable to be performed secondary to pacemaker), which did not reveal strokes. Episodes always occurred after activity and only upon sitting. His initial computed tomography angiogram (CTA) of the head and neck was unremarkable.
The important point for our purposes is that they do no represent myocardialinfarction. This gradual change in P wave morphology as the heart rate varies could be consistent with a wandering atrial pacemaker. Dr. Smith note: I wouldn't necessarily consider this ENTIRELY "benign."
100% occluded RCA with TIMI 0 flow Post drug-eluting stent placement with TIMI 3 flow While in the cath lab, she transiently developed complete heart block and became hypotensive requiring transvenous pacemaker placement and transient pressors. The transvenous pacemaker was removed the following day and pressors were not required again.
Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardialinfarction. I initially suspected V2 as being placed too high on the chest, but there is no accompanying inverted P wave here, so the positioning is sound. It’s important to stress the presence of a normal QRS (i.e.,
Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. IF treatment is needed ( because loss of the atrial "kick" results in hypotension ) — Atropine is the drug of choice ( in hope of speeding up the SA node to resume its pacemaking function ).
Immediate and early percutaneous coronary intervention in very high risk and high risk non-ST segment elevation myocardialinfarction patients. Diagnosis of ST-elevation myocardialinfarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Lupu et al.
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. AIVR is not always the result of significant pathology, but is classically associated with the reperfusion phase of acute myocardialinfarction. Do not treat AIVR. Am Heart J 1999;137:799–805.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Electrocardiographic Diagnosis of Acute Coronary Occlusion MyocardialInfarction in Ventricular Paced Rhythm Using the Modified Sgarbossa Criteria.
First degree heart block can also occur in a heart attack involving the lower part of the heart known as inferior wall myocardialinfarction. Complete heart block needs a temporary or permanent pacemaker depending on whether disease causing it is reversible or not.
For the outcomes, sensitivities were 85% for bleeding (comprehensive), permanent pacemaker implantation, and death. The kappa was higher in MA versus FFS for diabetes (P=0.03) and hypertension (P=0.025) but was lower in myocardialinfarction (P<0.0001).
CONCLUSIONS:Claims-based end points performed well in ascertaining death, disabling stroke, and pacemaker placement and were able to reproduce principal trial findings. CONCLUSIONS:Claims-based end points performed well in ascertaining death, disabling stroke, and pacemaker placement and were able to reproduce principal trial findings.
Oral anticoagulation also reduced a composite of cardiovascular death, all-cause stroke, peripheral arterial embolism, myocardialinfarction or pulmonary embolism (RR 0.85, 95% CI 0.73-1.00, We used random-effects models for meta-analysis and rated the quality of evidence using the GRADE framework. I2=0%; moderate-quality evidence).
Moreover, the improvement of care for patients with myocardialinfarction has resulted in higher survival rates, but as a result, more patients suffer from heart failure. This can be achieved by introducing electrodes into the vascular system which are connected to a pacemaker with a resynchronization function.
He received a permanent pacemaker during the subsequent inpatient stay. Detailed Considerations LBBB and MyocardialInfarction In the emergent setting it’s important to assess LBBB through the lens of the Smith-modified Sgarbossa criteria, especially in a context that is clinically consistent with Acute Coronary Syndrome.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). Some residual ischemia in the infarct border might still be present. Over the next couple of days the patient was weaned off of mechanical circulatory support.
The medics recorded the following initial ECG at time 0: The computer read (see below) gives no further comment beyond ventricular pacemaker. Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome.
When one of these arteries becomes completely blocked by a blood clot, it results in a heart attack, also known as MI (Myocardialinfarction). When a person experiences a heart attack or myocardialinfarction, they may feel chest pain and other symptoms in different parts of their body.
The researchers were able to show that those who had been ill with COVID-19 could also suffer from heart rhythm disturbances, both in the form of so-called tachycardias , when the heart ha rate is high, and bradyarrhythmias , when the heart is slow so that a pacemaker is sometimes needed.
Negative predictors of adverse outcome: Pacemaker Pre-syncope or "near-syncope," but there is still some small risk (5, 18) These last two are identified in studies, but I consider them dangerous signs and symptoms in their own right, as above: 10. QRS Old myocardialinfarction, 6. Syncope with Exertion (EGSYS) 7.
He had undergone coronary artery bypass grafting due to myocardialinfarction and severe three-vessel coronary artery disease. The patient underwent permanent dual chamber pacemaker implantation and reported no discomfort post-procedure. s (blue arrows; figure 1b ). And conduction resumes after an escape beat (yellow arrow).
2:34 PM, following right heart catheterization She then went into atrial fibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Acute myocardialinfarction triggered by emotional stress.
There are Q-waves in V1-V3 (myocardialinfarction of indeterminate age). So I am skeptical that this term has any practical significance. It is really simply a severe form of RBBB + LAFB, and we should all know by now what a terrible prognosis this combination confers. NOTE #1: Variations on this above "theme" of MBBB are common.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content