This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
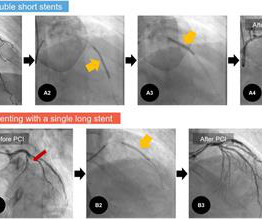
Objectives There is no consensus regarding the optimal choice between single long stent (SLS) and overlapped double short stents (DSS) in patients with acute myocardialinfarction (AMI). Therefore, we aimed to compare treatment outcomes among patients with AMI treated with these two different stenting methods.
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Smith: This is an enormous myocardialinfarction. This was stented with a 2.25 Next trop in AM.
Clinical success was defined as optimal stent expansion after final treatment with no in-hospital major adverse cardiovascular event (MACE). stent expansion at Maximum Calcium Site 96.7% Clinical Safety and Effectiveness Results: - 98.3% interventional cardiologist at ZNA Cardiovascular Center in Antwerp, Belgium.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. All three lesions had TIMI 2 flow prior to stenting. Because: 1) He has been reading this blog for a long time.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
As a low-volume PCI centre in the Middle East, we wanted to find out if the outcomes of our PCI procedures are different from those of high-volume PCI centres in the UK and the Western world. and the average number of stents 2.6. Prospectively collected data of all comers for PCI (urgent and elective) were retrospectively analysed.
Electrocardiographic Criteria to Differentiate Acute Anterior ST Elevation MyocardialInfarction from Left Ventricular Aneurysm. Smith : "What was the outcome?" Former resident: "Just saw cath report, LAD stent was 100% acutely occluded." They of course opened and stented it. You taught us well!"
In this study, we evaluate the safety and efficacy of TCAR in patients with symptomatic internal carotid artery disease compared with carotid endarterectomy (CEA) and carotid artery stenting (CAS).METHODS:A The primary outcomes included a 30-day stroke or transient ischemic attack, myocardialinfarction, and mortality.
Just before 10 AM, the patient received a stent to the culprit OM. Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). Peak troponin was 12 ng/mL. Guagliumi, G., Iwaoka, R.
The comparative effect of a combination of anticoagulant (AC) and antiplatelet (AP) versus AC monotherapy on clinical outcomes in patients with AF presenting with GIB is not well characterized. Patients with atrial fibrillation (AF) taking antithrombotic (AT) therapy are at increased risk of gastrointestinal bleeding (GIB).
A stent was placed. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. de Zwaan C.,
Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) and Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) integer scoring systems were tested.
BackgroundProcedural intravenous cangrelor has been proposed as an effective platelet inhibition strategy for stenting in acute ischemic stroke. Safety outcomes included rates of symptomatic intracranial hemorrhage, parenchymal hematoma type 2, petechial hemorrhage, and in‐stent thrombosis. 3.28];P=0.836). versus 0%;P=0.911).ConclusionCangrelor
An open 90% LAD was stented. Here is the ECG the next AM: There was so little infarction that there are lateral, but no anterior reperfusion T-waves (normally, there would be Wellens' type waves after LAD reperfusion). Relationship of TIMI myocardial perfusion grade to mortality after administration of thrombolytic drugs.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Yet this is rarely followed, and patient outcomes like this are the result once in a while. Am J Emerg Med. 2014;32:e5–e8.
The primary outcomes included 30-day combined stroke and transient ischemic attack (TIA), myocardialinfarction (MI), and mortality. The primary outcomes included 30-day combined stroke and transient ischemic attack (TIA), myocardialinfarction (MI), and mortality. This was explained in Figure 1.Results:A
The ECG is diagnostic of occlusion myocardialinfarction (OMI). This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP. Patient #3 — turned out to have myocarditis.
Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. Such an escape would have a wider complex.
Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi). It was stented.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily. Here is the time-zero 12 Lead ECG.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. Prospective validation of current quantitative electrocardiographic criteria for ST-elevation myocardialinfarction. Int J Cardiol 2019 2. -- Meyers HP, Bracey, Smith et al.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
LAD and D1 were stented, but flow unfortunately could not be well restored despite efforts (they list the post intervention TIMI flow still as 0). Serial tracings following stent placement confirmed the large extent of myocardial injury. LCX and RCA were described as "normal" in the cath report. Am J Emerg Med. 2021.11.023.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Notice also that there is new T-wave inversion in III with upright T-wave in aVL, confirming inferior infarction.
This is diagnostic of myocardialinfarction. The lesion was stented. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. Int J Cardiol. 2016.01.188.
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). Here is the angiogram after stent placement. The patient suffered a large infarct. St depression in lead AVL differentiates inferior st-elevation myocardialinfarction from pericarditis. Circulation , 130 (25).
Background Drug-eluting stents (DESs) have become the gold standard of coronary angioplasty since their inception in 2002. We aimed to compare outcomes between a broad range of second-generation DP-DES and BP-DES in an all-comer population. vs 57.5%, p=0.010), a greater average number of stents implanted per patient (1.72±0.92
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Association between opioid analgesia and delays to cardiac catheterization of patients with occlusion MyocardialInfarctions. A single DES stent was placed, and the patient did well post-procedure. Abstract 556.
They were stented. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. Available from: [link] Excerpt: "To illustrate the limitations imposed by sample size, recent data from our institution reveal that we identify approximately 225 type I myocardialinfarctions (MI) in a typical year.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. After many hours, the decided that it was appropriate to do an angiogram and they found a distal LAD occlusion which was opened and stented. Outcome The cath lab was activated by the emergency physician.
This case was texted to me by one of our residency graduates, and with the outcome, so I don't know how I would have interpreted it blindly. It was opened and stented. Comparison of the QRS Complex, ST-Segment, and T-Wave Among Patients with Left Bundle Branch Block with and without Acute MyocardialInfarction.
Left main coronary artery disease (CAD) and diabetes pose significant challenges in cardiovascular care, often leading to adverse outcomes. Preliminary evidence from trials focusing on patients with multivessel disease has hinted at diabetes as a potential modifier of treatment outcomes.
Aims To estimate the 1-year cost-effectiveness of stepwise provisional versus systematic dual stenting strategies. Aims To estimate the 1-year cost-effectiveness of stepwise provisional versus systematic dual stenting strategies. Uncertainty was explored by probabilistic bootstrapping.
suggest that the drug-coated balloon offers an effective treatment strategy for the management of coronary in-stent restenosis, or blockages recurring within previously placed stents. Smith Center for Outcomes Research in Cardiology and section chief of Interventional Cardiology at BIDMC. percent).
This systematic review of the literature aims to explore outcomes in the patients treated with conservative management vs. invasive strategy. of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% Approximately 48.5% The overall reported in-hospital and follow-up mortality rates were 1.2%
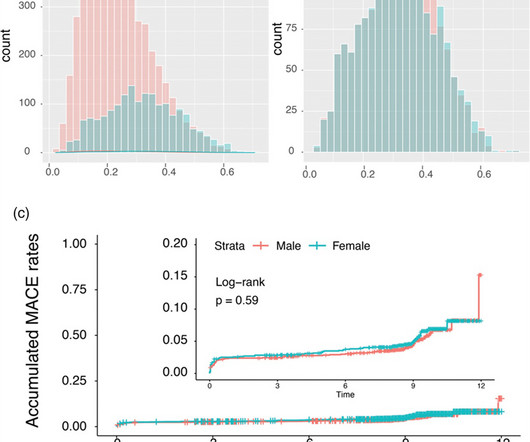
Background: Gender-specific outcomes after percutaneous coronary interventions were studied by a number of research groups with different endpoints and cohorts of different ethnic extractions. Materials and methods: The basis for this post hoc analysis was two large all-comers studies with prospectively enrolled patients from Europe and Asia.
Background For high bleeding-risk patients (HBR) undergoing percutaneous coronary intervention (PCI), the LEADERS FREE (LF) and LEADERS FREE II (LF II) trials established the safety and efficacy of a stainless steel polymer-free biolimus-coated stent (SS-BCS) with 30 days of dual antiplatelet treatment (DAPT). to 9.2%) patients.
BACKGROUND:We previously reported the use of minimal stent area to predict angiographic in-stent restenosis after drug-eluting stent implantation for unprotected left main (LM) disease. Circulation: Cardiovascular Interventions, Volume 17, Issue 1 , Page e013006, January 1, 2024. mm2for distal LM (area under the curve, 0.57;P=0.15),
The 2 coprimary outcomes were target lesion revascularization and myocardialinfarction. The secondary outcomes included ischemia-driven target lesion revascularization, target vessel myocardialinfarction, death, cardiac death, target vessel revascularization, stent thrombosis, and major adverse cardiac events.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Accessed May 2024. Kirtane, Yongjian Wu, William Wijns, Weixian Yang, Martin B. Leon, Shubin Qiao, Gregg W.
The primary outcome was the composite occurrence of stroke, myocardialinfarction, and allcause death following carotid revascularization. A multivariate Cox regression analysis was conducted to assess the primary outcomes. years, 4087 patients experienced a primary outcome. Over a mean followup period of 4.133.14
Background Bioresorbable vascular scaffolds (BVS) were designed to reduce the rate of late adverse events observed in conventional drug-eluting stents (DES) by dissolving once they have restored lasting patency. All other outcomes were statistically equivalent. to 1.70; p=0.01) resulting from high rates of TVMI and ID-TLR.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content