This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardialinfarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
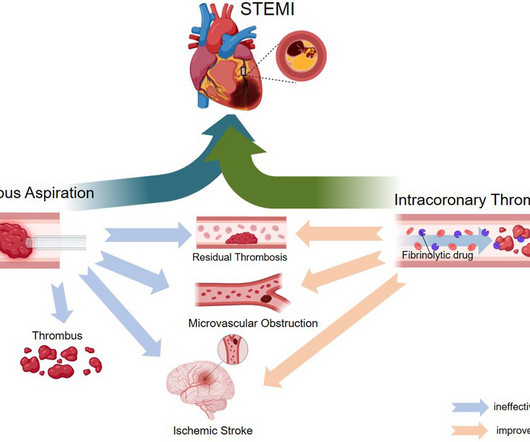
ST-elevation myocardialinfarction (STEMI) is a critical cardiovascular emergency characterized by acute coronary artery occlusion and subsequent myocardial injury. However, despite successful revascularization, microvascular obstruction (MVO) remains a major challenge, contributing to adverse clinical outcomes.
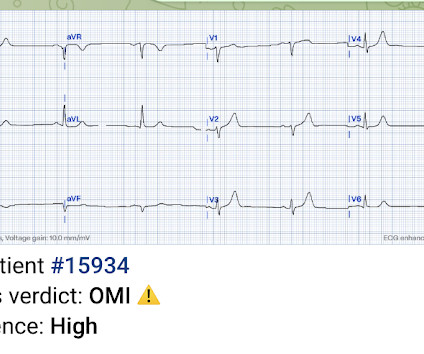
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." The case continues. Worrall, C.,
What is the impact of complete revascularization versus culprit-only revascularization on outcomes in older patients with ST-segment elevation myocardialinfarction (STEMI) and non–ST-segment elevation myocardialinfarction (NSTEMI)?
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients.
What are the outcomes of bivalirudin vs. heparin anticoagulation during percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardialinfarction (STEMI)?
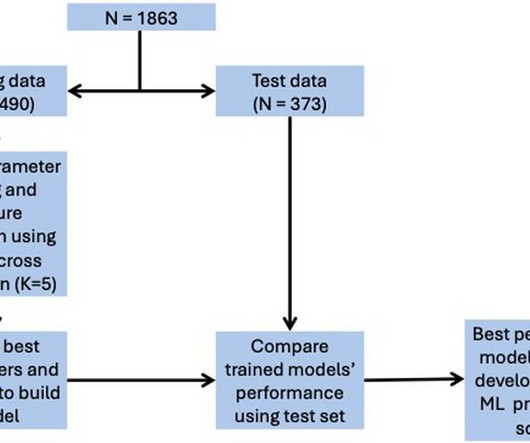
We developed a user-friendly web application for real-world use, yielding risk scores as a percentage.ConclusionsThe STEMI-ML score effectively predicts in-hospital outcomes in STEMI patients and may assist with risk stratification and individualising patient management.
(MedPage Today) -- ATLANTA -- Fractional flow reserve (FFR)-guided complete revascularization in patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel coronary artery disease did not result in better outcomes compared.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Opiates are associated with worse outcomes in MyocardialInfarction.
BackgroundThe pharmacoinvasive (PhI) strategy is the standard-of-care for ST-elevation myocardialinfarction (STEMI) patients when primary percutaneous coronary intervention (pPCI) is unfeasible. Multivariable logistic regression models were used to assess the association between lysis-PCI timing and outcomes.
Background Despite restoration of epicardial blood flow in acute ST-elevation myocardialinfarction (STEMI), inadequate microcirculatory perfusion is common and portends a poor prognosis. The primary outcome was major adverse cardiac events (MACE). to 3.28; I 2 =0%; p=0.67; minor bleeding, RR=1.47; 95% CI 0.90
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
It is now well known that even if a coronary artery is opened well after a myocardialinfarction, with good flow in the epicardial coronary arteries, there could be impaired myocardial perfusion. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. J Am Coll Cardiol. van Leeuwen, Stephen P.
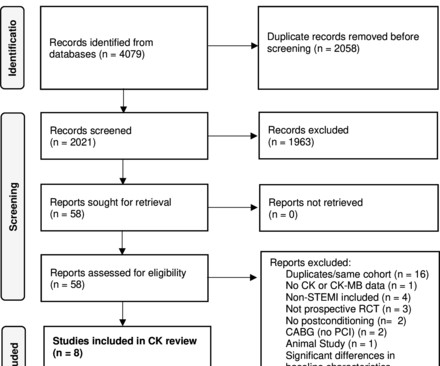
Objectives This study aimed to perform a meta-analysis of the short-term impact of ischaemic postconditioning (IPoC) on myocardial injury in ST elevation myocardialinfarction (STEMI) using surrogate cardiac biomarkers. Few studies used troponin as an outcome, thus, a subanalysis of troponin dynamics was not performed.
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel coronary disease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
However, its prognostic role following percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI) remains unclear. Echocardiography was performed upon admission and at 6 months post-myocardialinfarction (MI). vs. 6.231.91, P 8.13
Stress hyperglycemia ratio (SHR), associated with adverse outcomes in patients with ST-segment elevation myocardialinfarction (STEMI), has several definitions. This study aims to assess the prognostic value o.
Background Despite improvements in outcomes of ST elevation myocardialinfarction (STEMI), ventricular septal rupture (VSR) remains a known complication, carrying high mortality. The contemporary incidence, mortality, and management of post-STEMI VSR remains unclear.
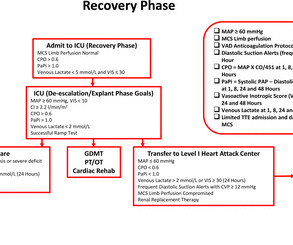
Introduction Cardiogenic shock (CS) complicates 5%–15% of cases of acute myocardialinfarction (AMI) with inpatient mortality greater than 40%. The implementation of standardised protocols may improve clinical outcomes in patients with AMI-CS.
Background and objectivesThe optimal timing for complete revascularization (CR) in patients with acute myocardialinfarction (AMI) and multivessel disease (MVD) remain uncertain.MethodsThis post-hoc analysis of the FRAME-AMI trial included AMI patients with MVD (n=549). Other secondary endpoints were also not significantly different.
This systematic review of the literature aims to explore outcomes in the patients treated with conservative management vs. invasive strategy. of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% Approximately 48.5%
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
European Heart Journal , ehy651, [link] Published: 26 October 2018 [link] Timing of revascularization in patients with transient ST-segment elevation myocardialinfarction: a randomized clinical trial. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded.
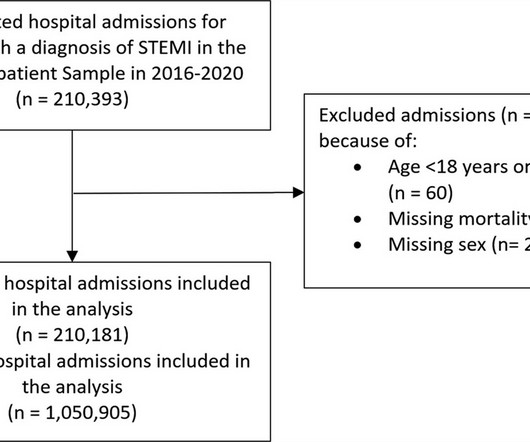
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardialinfarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% reduction in admissions in 2020. reduction in admissions in 2020.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Could it be acute (vs. subacute or days old)?
The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. Been discharged to home with potential disastrous outcome. Undergone stress test with uncertain results. Learning Points 1.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardialinfarction (STEMI).Objective:Our years, 53 women) followed for up to 15 years.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Could it be acute (vs.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Smith: This is an enormous myocardialinfarction. Most large STEMI have peak troponin I in the 20.0 Next trop in AM. Peak trop 257.97
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. Do you need posterior leads? If so, how will they change management?
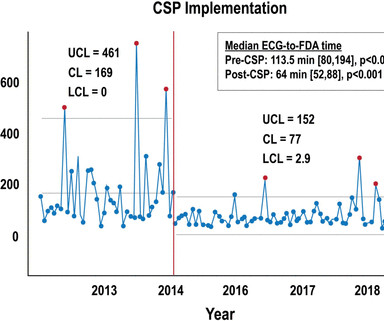
Background Patients who experience in-hospital ST-segment elevation myocardialinfarction (iSTEMI) represent a uniquely high-risk cohort owing to delays in diagnosis, prolonged time to reperfusion and increased mortality. Key metrics and clinical outcomes were compared before and after CSP implementation.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardialinfarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
Aim Acute injury and subsequent remodelling responses to ST-segment elevation myocardialinfarction (STEMI) are major determinants of clinical outcome. Current imaging and plasma biomarkers provide delayed readouts of myocardial injury and recovery.
A meta-analysis was performed on primary outcomes of major adverse cardiac events (MACE) and all-cause mortality. A meta-analysis was performed on primary outcomes of major adverse cardiac events (MACE) and all-cause mortality. Heterogeneity was examined with I2statistics. vs 6.0%), stroke (RR=1.02; 95% CI [0.38, 2.75]; p =0.97; 2.0%
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? The patient stabilized and had a good outcome. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 The corrected QT interval is extremely long, about 500 ms. If the patient is at 1.8,
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. Zwolle MyocardialInfarction Study Group.
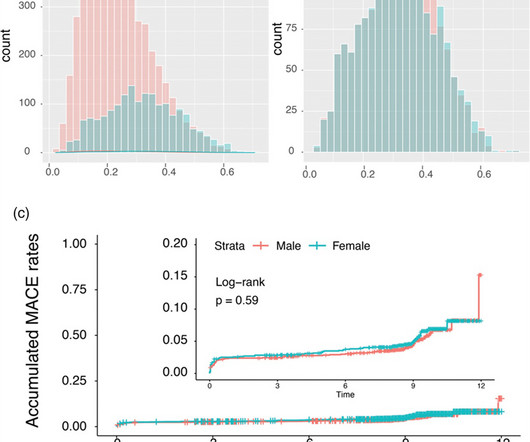
Background: Gender-specific outcomes after percutaneous coronary interventions were studied by a number of research groups with different endpoints and cohorts of different ethnic extractions. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 3.9%; P = 0.020).
Introduction:Elevated LDL cholesterol is linked to microvascular injury and adverse cardiac events in STEMI patients. This study examines the impact of prior statin use on LDL levels at the time of MI, focusing on NSTEMI and STEMI patients. For STEMI, the treated group had an average LDL level of 87.8 ± 42 mg/dL versus 103 ± 41.2
Angiogram: "ACS - Non ST Elevation MyocardialInfarction. Meyers note: notice in their documentation many of the classic mistakes of the STEMI generation: "Non ST Elevation MI" as their reasoning for why the patient did not merit emergent reperfusion, while simultaneously calling it "emergently" (after 8 hours!!!)
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty.
associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. MINOCA I do not have the bandwidth here to write a review of MINOCA.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. AIVR is not always the result of significant pathology, but is classically associated with the reperfusion phase of acute myocardialinfarction. Is there STEMI? The patient continued having chest pain. Moffat, M.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content