This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
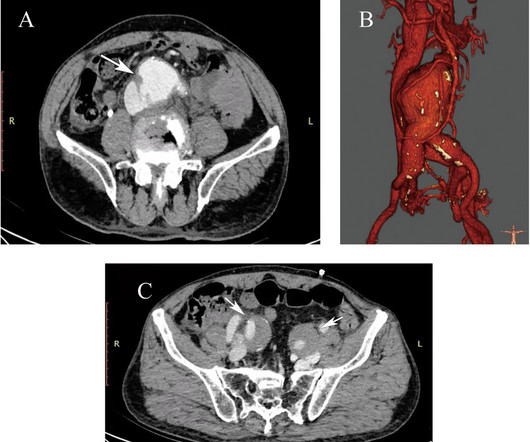
Endovascular stent graft repair represents a practical approach to managing this fatal condition.Case presentationA 75-year-old male patient was admitted to the nephrology department of our hospital, complaining of acute back pain, hematuria, and repeated vomiting for one week.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. The patient's laboratory studies revealed troponin mildly elevated at 25 ng/L but liver enzymes, lipase were normal. It is stented with good angiographic result.
Such medium or distal arterial segments have not been assessed with respect to thrombectomy devices used during endovascular therapy. Arterial diameters were measured at all these sites.
BACKGROUND:Geographic stent-ostium mismatch is an important predictor of target lesion failure after percutaneous coronary intervention of an aorto-ostial right coronary artery lesion. Optimal visualization of the aorto-ostial plane is crucial for precise stent implantation at the level of the ostium.
Conventional coronary angiograms are obtained by injecting medications directly into the coronary arteries and imaging them with X-ray equipment in cardiac catheterization laboratory. CT coronary angiogram is also useful to evaluate coronary artery bypass vein grafts and larger coronary stents.
All these factors, again, support an ECG diagnosis of LVH The patient was nonetheless taken for emergency angiography, and a 99% mid-LAD lesion was found and stented. Electrocardiograhic findings resulting in inappropriate cardiac catheterization laboratory activation for ST-segment elevation myocardial infarction. Am J Cardiol.
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. That the regular WCT in ECG #1 was not VT was subsequently established — because EP study could not induce VT in the laboratory. Home medications included metoprolol, but no calcium- or sodium-channel blocking agents.
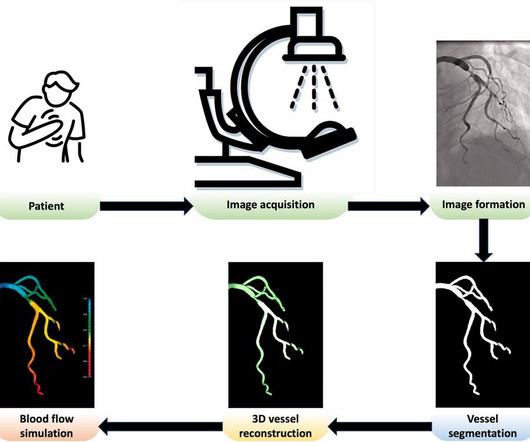
With this type of procedure, blood flow in coronary arteries is viewed in real-time, making it possible to detect stenoses precisely and control percutaneous coronary interventions and stent insertions.
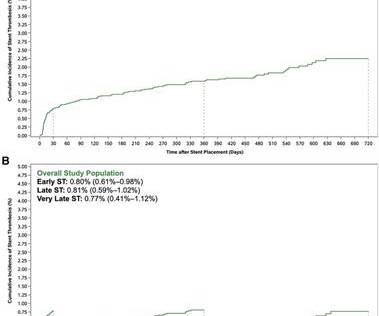
Background Stent thrombosis (ST) is an uncommon but serious complication of stent implantation. Methods The analysis included patients who received stent placement for the index acute coronary syndrome (ACS). drug-eluting stent (DES) vs. bare-metal stent (BMS) and anticoagulant with rivaroxaban vs. placebo].
suggest that the drug-coated balloon offers an effective treatment strategy for the management of coronary in-stent restenosis, or blockages recurring within previously placed stents. In particular, patients with multiple prior stents have very poor long-term outcomes. This study was supported by Boston Scientific Corp.
Routine coronary angiography with percutaneous coronary intervention (PCI) is often deferred in the presence of laboratory markers of acute inflammation to prevent complications. In total, 11 327 patients underwent PCI and of those, 6880 patients had laboratory results available. for stable ischemic heart disease. P<0.001).ConclusionsAn
Coulter Department of Biomedical Engineering and director of the Cardiovascular Fluid Mechanics Laboratory at Georgia Tech. A novel flexible stented blood inlet will conform to the shape of the patient’s heart to prevent flow stasis and clotting. The overall effort will be led by principal investigator Lakshmi P.
narrates and is a co-producer of a documentary focused on radiation and orthopedic injuries suffered by doctors and nurses who work in cardiac catheterization laboratories where they apply the very latest non-surgical technologies to treat the world’s leading cause of death, heart disease. Rizik , M.D.,
Results are adjudicated by an independent Imaging Core Laboratory and a Clinical Events Committee. In-stent stenosis occurred in 2.2% (17) and was associated with fusiform morphology at 1 year FU (OR, 4.82, 95% CI, 1.28 -14.35; p=0.018).Conclusion:Treatment Fusiform morphology was associated with in-stent stenosis.
This was stented. Be certain that your laboratory value is accurate and that it corresponds with the ECG findings! After pacing, there was no recurrence of Torsades. After resuscitation, he was found to have a 90% thrombotic lesion in the same saphenous vein graft to the right posterior descending artery. The patient stabilized.
Late-Breaking Science sessions and concurrent oral abstract presentations are as follows: Wed., MT) TESLA: The Thrombectomy for Emergent Salvage of Large Anterior Circulation Ischemic Stroke Trial: 1-Year Outcome: Osama Zaidat, Mercy Health St. 8 Late-Breaking Science Oral Abstracts III (beginning at 2:00 p.m.
A completely blocked artery is located, a wire is inserted through it, the clot is sucked, the narrowing is widened with a balloon, and then a stent (stainless steel wire mesh) is placed to maintain consistent flow. Coronary angiography is performed under local anesthesia using the right arm without any cuts.
Total proximal LAD occlusion was found and stented at angiography soon after the ECG above. Troponin I quickly exceeded the laboratory limit of reporting at 25,000 ng/L. Here are some images: Next morning ECG: Reperfusion findings are clear. 4 days later: Continued reperfusion.
ECG at 11 hours: No comment needed Given this EKG with diagnostic findings, his heparin infusion was stopped, and he was given a 5000 unit heparin bolus and 180 mg of ticagrelor while the cardiac catheterization laboratory was activated and interventional cardiology was emergently consulted.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content