This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. Do you need posterior leads? If so, how will they change management?
7, 2024 — The Society for Cardiovascular Angiography & Interventions (SCAI) recently announced the publication of the Expert Consensus Statement on the Management of Patients with STEMI Referred for Primary PCI. tim.hodson Mon, 10/07/2024 - 14:45 Oct.
She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. Back to the case: Unfortunately, the ECG was not understood by the provider.
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH? The criteria of Armstrong et al. References 1.
He called 911 and paramedics recorded a prehospital 12 lead ECG which showed a clear inferior STEMI (not shown, tracing could not be found). Objectives : To find the incidence of any rSTD or T-wave inversion (TWI) in angiographically proven inferior STEMI. No true STEMI had absence of reciprocal depression in lead aVL.
Standard baseline variables were collected for both groups, whereas for AMI patients, laboratory and psychological tests were also carried out. Among AMI patients, there was no difference in the rate of cortisol increase between STEMI and NSTEMI patients (time-group interaction P=0.841).
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." As was the more reliable laboratory troponin T (0.00 See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. Of the 418 patient with ACO, 29% did not meet “STEMI criteria.”
Department of Laboratory Medicine, Hennepin County Medical Center; Professor, University of Minnesota School of Medicine Stephen W. Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. Apple, Ph.D.
In fact, there is laboratory evidence that CO toxicity increases Plateletneutrophil aggregates and plasma myeloperoxidase (MPO) concentration and thus may precipitate ACS (though this is by no means clinically proven). An ECG is always recorded for CO toxicity. This was his ECG.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Background Despite the crucial role of Chest pain centers (CPCs) in acute myocardial infarction (AMI) management, China's mortality rate for ST-segment elevation myocardial infarction (STEMI) has remained stagnant. Conclusion CPC quality control metrics affect STEMI mortality based on Killip class.
Attempts to decrease the time from diagnosis of ST-segment elevation myocardial infarction (STEMI) to arrival at the catheterization laboratory have been extensively investigated. However, strategies during the procedure aiming to reduce the time to reperfusion are lacking. We searched PubMed, Embase, and Cochrane Central.
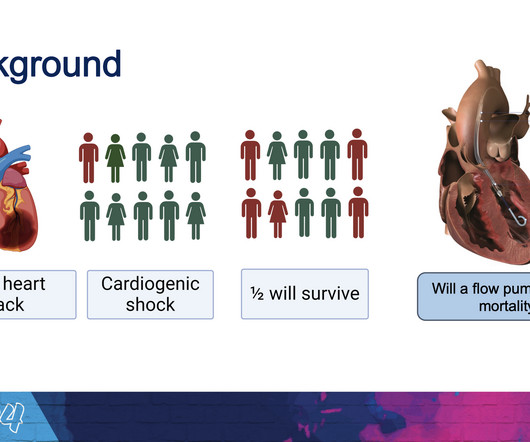
The new trial, called DanGer Shock , is the first trial powered to examine whether the use of micro-axial flow pumps can improve survival in ST-elevation myocardial infarctions (STEMI, the most serious type of heart attack) that are complicated by cardiogenic shock. Among 355 patients who were included in the analysis, 58.5%
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Based on his clinical presentation and laboratory findings, rhabdomyolysis was suspected to be the etiology of his hyperkalemia. From Ken Grauer ( See below ) — with this Figure adapted from LITFL. They opined that the ECG could instead be "metabolic."
The patient was given aspirin 325 mg and laboratory workup was initiated. Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative. Angiogram is shown below.
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it. He was sent back to the waiting room, where he suffered a VF arrest.
The first EKG was concerning for a Wellen’s-like pattern of subtle reperfusion changes in the setting of stuttering anginal-equivalent symptoms, but none were diagnostic of STEMI or OMI. Later in the night, the patient became bradycardic and developed a Mobitz II pattern , but he remained asymptomatic and hemodynamically stable.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content