This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
METHODS:The AHA, through its Epidemiology and Prevention Statistics Committee, continuously monitors and evaluates sources of data on heart disease and stroke in the United States and globally to provide the most current information available in the annual Statistical Update with review of published literature through the year before writing.
METHODS:The AHA, through its Epidemiology and Prevention Statistics Committee, continuously monitors and evaluates sources of data on heart disease and stroke in the United States and globally to provide the most current information available in the annual Statistical Update with review of published literature through the year before writing.
The primary outcome was a composite of inhospital adverse events. Associations between multimorbidity patterns and outcomes were evaluated using multivariableadjusted logistic regression models. years]) admitted to the China Chest Pain Center Database between 2016 and 2021. Among 9570 patients, 50% (n=4789) had multimorbidity.
A new joint guideline from the American Heart Association (AHA), the American College of Cardiology (ACC) and nine other medical societies reports early diagnosis and treatment of peripheralarterydisease is essential to improve outcomes and reduce amputation risk, heart attack, stroke and death for people with PeripheralArteryDisease (PAD).
The primary outcome was a 3-year major bleeding event defined as moderate or severe bleeding according to the Global Use of Streptokinase and t-PA for Occluded Coronary Arteries bleeding criteria. Conclusions These findings suggest that BP management is essential to prevent bleeding events after PCI.
Prevalence of hypertension (86.6%), heart failure (22.7%), diabetes (54.8%), chronic kidneydisease (23.6%), and chronic obstructive pulmonary disease (35.4%) was high. Ongoing studies will yield important insights regarding improving care and outcomes in this highrisk group. At 1 year, 9.4% of patients had died.
Because CMHC is committed to forging relationships with organizations that share a pursuit of bettering patient outcomes through unparalleled provider education, many like-minded regional and national organizations will be in attendance.
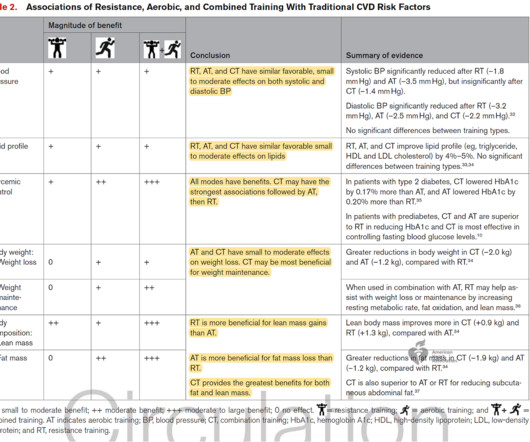
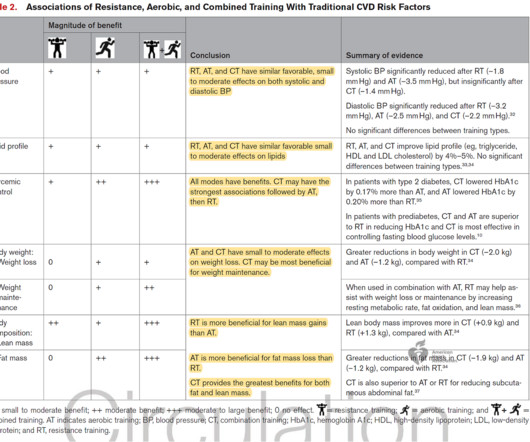
Participating in any resistance training is associated with a 15%–17% lower risk for these outcomes compared to non-participation. Most data suggest that 30–60 minutes per week is sufficient to maximize the risk reduction — benefits start to plateau and then reverse after this threshold.
Participating in any resistance training is associated with a 15%–17% lower risk for these outcomes compared to non-participation. Most data suggest that 30–60 minutes per week is sufficient to maximize the risk reduction — benefits start to plateau and then reverse after this threshold.
5 Over my career as a cardiovascular surgeon, as well as an immunologist, I have witnessed how current treatments for ASCVD have led to considerable improvements in outcomes, yet many patients remain vulnerable to life-threatening cardiac events.1,6 22 In general, hsCRP values above 2.0 34 The safety of colchicine, 0.5 μ/L on 0.6
AF is associated with an increased risk of death as well as multiple adverse outcomes, including stroke, cognitive impairment or dementia, myocardial infarction, sudden cardiac death, heart failure (HF), chronic kidneydisease (CKD), and peripheralarterydisease (PAD). million.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content