This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- The FDA approved the Esprit BTK everolimus-eluting scaffold system for chronic limb-threatening ischemia (CLTI) below the knee, Abbott announced on Monday. This system represents the first drug-eluting resorbable scaffold with.
Smits and a distinguished team of international researchers, the trial compares the performance of SMT's biodegradable-polymer sirolimus-eluting Supraflex Cruz stent with the biodegradable-polymer Ultimaster Tansei * stent in patients with high bleeding risk (HBR) undergoing abbreviated dual antiplatelet therapy (DAPT).
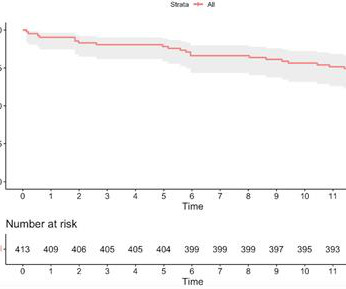
Introduction The use of contemporary drug-eluting stents (DES) has significantly improved outcomes of patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI). cases, the target lesion was in-stent restenosis (ISR). At 1 year, only two (0.5%) subjects presented ischemia-driven TLR.
In this phenomenon, a thrombus forms within the lumen of the stent graft component of the frozen elephant trunk prosthesis and puts the patient at risk for downstream embolization with visceral or lower limb ischemia. Therefore, the presence of ILT is associated with increased short-term mortality and morbidity.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. 4 Recent literature has reported clinical benefits associated with rescue stenting in the setting of ICAD‐related MT‐refractory strokes.5
(MedPage Today) -- For patients with peripheral artery disease (PAD) and chronic limb-threatening ischemia, drug-eluting stents and drug-coated balloons did not improve amputation-free survival compared with balloon angioplasty alone in the BASIL.
Of note, patient had a with left cavernous‐ICA stent placement a month before the presentation and was noncompliant to antiplatelets. We described a left intracranial ICA flow diversion occlusion without anterior circulation ischemia and left PCA ischemia demonstrated. In the emergency department (ED), her NIHSS was 28.
No ischemia. This is a conundrum, because it is clear that the patient is having an acute MI, the ECG is dynamic, but the pain is very mild and there is no ECG evidence of active transmural ischemia. We already know that the ischemia is ongoing, though mild (because of the persistent pain). The culprit was opened and stented.
Herein, we describe a single‐step approach to deploy Neuroform Atlas stent (Stryker Neurovascular, Fremont, CA) which is a hybrid laser‐cut, nitinol self‐expanding stent without the need for ELW or lesion re‐access using MINI TREK RX (Abbott Vascular, Inc., There was no restriction on time from last known well (TLKW) to MT.
BackgroundThe rapid evolution of artificial intelligence (AI) in conjunction with recent updates in dual antiplatelet therapy (DAPT) management guidelines emphasizes the necessity for innovative models to predict ischemic or bleeding events after drug‐eluting stent implantation.
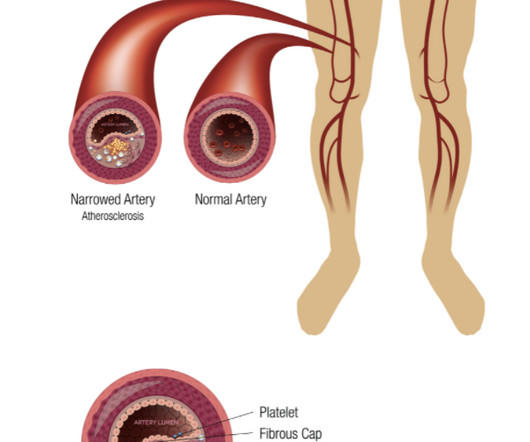
Coronary heart disease is a narrowing or obstruction of the vascular cavity caused by atherosclerosis of the coronary arteries, which leads to myocardial ischemia and hypoxia. At present, percutaneous coronary intervention (PCI) is an effective treatment for coronary atherosclerotic heart disease.
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
He interprets here: "This EKG is diagnostic of right bundle branch block and transmural ischemia of the anterior wall, most likely from an occlusion of the proximal LAD. There was a 100% proximal LAD occlusion that was opened and stented. It was recorded at 0530: What do you think? The young ED tech immediately suspected LAD OMI.
To our knowledge, no studies have directly compared the right and left TRA for carotid artery stenting (CAS). However, in interventional cardiology, the left TRA has demonstrated clear clinical benefits, particularly for right-handed patients. All carotid stenoses were successfully dilated.
The Freesolve BTK RMS is designed for individuals suffering from chronic limb-threatening ischemia (CLTI). Updated estimates for the burden of chronic limb-threatening ischemia in the Medicare population, Journal of Vascular Surgery, Volume 77, Issue 6, 2023, 1760-1775 2 Seguchi M., 2,3 It has shown 99.6%
Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. non-occlusive ischemia) Ongoing ischemic symptoms in NSTEMI is already an indication for emergent cath, regardless of the ECG. Peak troponin was not recorded. The patient survived the hospitalization.
Diseased human arteries are most simply, reliably, and successfully treated with drug-eluting, balloon-expandable stents," said Lewis B. 2 An estimated 10% of patients with PAOD have its most severe form: chronic limb-threatening ischemia (CLTI). Eur J Vasc Endovasc Surg. 2012;43:55-61. J Am Heart Assoc. DOI: 10.1161/JAHA.118.009724.
IVUS Measurements Measurements include the measurement of lumen, plaque, calcium, remodeling, stent length and volumetric measurements. It can also give guidance for stenting in terms of assessment of stent apposition and good expansion. Incomplete stent apposition can be detected by intravascular ultrasound.
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
ObjectiveSpinal cord ischemia due to damage or occlusion of the orifices of aortic segmental arteries (ASA) is a serious complication of open and endovascular aortic repair. Furthermore, it aids in planning and conducting safe aortic intervention and assists in deciding on single- or two-staged stent graft procedures.
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Cath days later showed complete occlusion of the LAD, stented. Ultimately, cardiac cath was done in Case #2, with stenting of the "culprit" LAD lesion.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
BackgroundMyocardial ischemia can impair the speed and intensity of myocardial contractility, frequently undetectable by conventional echocardiography in early stages. A cutoff value of 26.9% for LVEF1 had a sensitivity of 89.5% and specificity of 83.9% for predicting coronary artery stenosis 70%.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI.
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. Subendocardial ischemia does not localize. Finally the OMI was realized.
He underwent coronary stenting (uncertain which artery). Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chest pain are nearly diagnostic of ischemia. Ischemia on the ECG can be very subtle and is easily missed. Lesson : 1.
I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. What would I expect the angiogram to show?
Of the 32 patients, 9(28.1%) had dissection with diagnostic angiograms, 6(18.8%) endovascular thrombectomy, 15(46.9%) aneurysm treatment, and 2(6.3%) angioplasty with or without stenting. Only 4(12.5%) were treated with hyperacute stenting. One patient was symptomatic with neck pain. The median duration of acute treatment was 3 months.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. The OM-1 was opened and stented, then the LAD was stented 3 days later. There is no ST elevation. How can we tell the difference?
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
Answer : There is very abnormal T-wave inversion in aVL which is typical of subtle transmural/subepicardial (due to occlusion) ischemia to the inferior wall. Similarly, the precordial T-wave inversions in V2-V4 are reciprocal to posterior wall transmural/subepicardial (due to occlusion) ischemia. An 80% thrombotic RCA was stented.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3. Lessons: 1.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? The last echocardiography 12 months ago showed HFmrEF.
In his four months follow up clinic visit he had no further concerns of recurrent strokes or new symptoms.ResultsCarotid stump syndrome is a rare cause of cerebral and retinal ischemia; however, it must be considered in patients with recurrent ischemic strokes and chronic ipsilateral ICA occlusion.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
Thus, there are some suspicious abnormalities, but no definite signs of ischemia. Because of persistent symptoms, another ECG was recorded 30 minutes later: There is only one new finding on this ECG which suggests ischemia. The difference is significant and highly suggests posterior ischemia. It is very subtle but real.
This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. Perusal of her charts revealed that she had an LAD stent that was very close to the ostium of the circumflex. A right sided ECG was recorded 3 minutes later. This is her ECG 1.5
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. Peak troponin was 12 ng/mL.
LAD: severe in-stent restenosis in the mid (80%) and distal (90%) segment and diffuse disease distally. Ramus intermedius: large, severe in-stent restenosis at the distal stent edge (90%) and severe de-novo stenosis at the ostial segment (90%). The pain did not resolve with NTG, and so he went to emergent angiography: 1.
Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So there is now high pre-test probability + refractory ischemia + Modified Sgarbossa + dynamic ECG changes. So the RCA was stented. Learning points 1.
It means either a percutaneous coronary intervention with a stent or CABG. Reference : Apart from the heavily quoted classics of COURAGE, BARI-2D, ISCHEMIA, ORBITA 1 etc. You may be. But I am not.You need to undergo some re-vascularisation procedure. What do you mean by that Doctor ? No we can’t.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content