This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Ischemia with no obstructive coronary arteries (INOCA) is an increasingly recognized condition in patients presenting with angina and positive stress tests but without significant coronary artery stenosis.
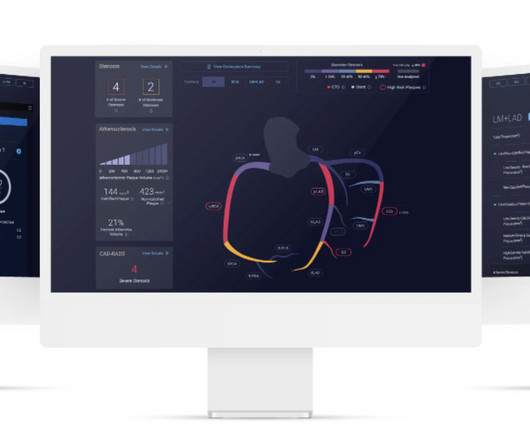
milla1cf Tue, 01/09/2024 - 11:32 January 9, 2024 — Cleerly , the company working to create a new standard of care for the diagnosis of heart disease, announced the launch of Cleerly ISCHEMIA , which recently received U.S. Cleerly ISCHEMIA is a transformative addition poised to reshape the landscape of cardiac care.”
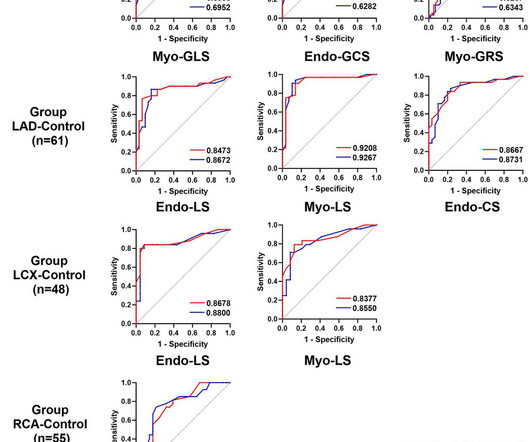
Receiver operator characteristic curve (ROC) analysis indicated that CTFFR were effective in diagnosing impaired myocardial strain, particularly LS.ConclusionThere is a strong correlation between CTFFR, which is a functional measure for assessing coronary artery stenosis, and myocardial strain.
This confirms that the pain was ischemia and is now resovled. Because the pathologist determines the degree of stenosis by dividing the lumen area by the total area, the degree of stenosis will be overestimated. The angiographer uses a denominator that is too small, thereby underestimating the degree of stenosis.
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. Type I ischemia. He was taken to the Cath Lab.
The study describes the validation of Cleerly's artificial intelligence-guided quantitative coronary CT angiography (AI-QCT) ISCHEMIA technology for diagnostic accuracy and prognostic risk stratification. High Diagnostic Accuracy of AI-ISCHEMIA in Comparison to PET, FFR-CT, SPECT, and Invasive FFR: A Pacific Substudy. 2024.01.007.
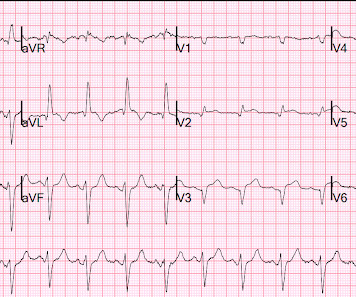
At the hospital, left main coronary-artery stenosis was seen on angiography (shown in a video). In a 57-year-old man with chest pain, an ECG obtained by EMS showed widespread ST-segment depressions.
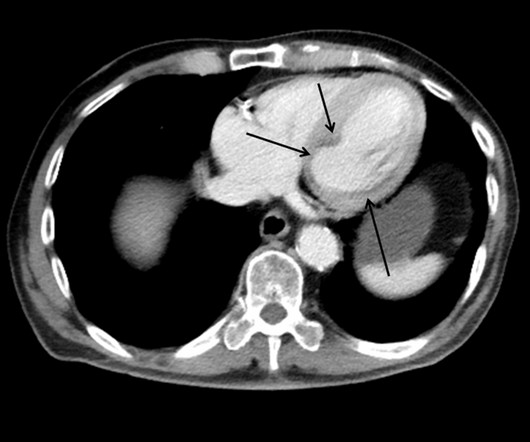
This case shows a CT image of subendocardial ischemia. The post cath ECG was not recorded until the next morning: The ischemia is almost entirely resolved. The inferior and posterior walls are also at chronic risk of subendocardial ischemia because of this tenuous blood supply. No evidence for watershed ischemia.
Such a pattern is consistent with significant left main coronary artery stenosis. Angiography done after initial stabilization showed severe stenosis of distal left main coronary artery. ST segment elevation in aVR in proximal LAD occlusion before first septal is thought to be due to transmural ischemia of the basal part of the septum.
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP?
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Diagnosis and treatment of ischemia-producing coronary stenoses improves 5-year survival of patients undergoing major vascular surgery.”
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
High Diagnostic Accuracy Of AI-Ischemia in Comparison To PET, FFR-CT, SPECT, and Invasive FFR: A PACIFIC Sub-Study. Derivation, Validation and Prognostic Assessment of an AI-Based Algorithm for Determination of Coronary Ischemia: The CREDENCE and PACIFIC Trial. In Press European Heart Journal CV Imag 2024.This James Min, M.D.
Myocardial ischemia may induce myocardial fibrosis, a condition that progressively leads to ventricular remodeling, heightening the risk of heart failure. 68 Ga-FAPI-04 PET/CT shows promise in assessing fibroblast activation in patients with early myocardial infarction characterized by prolonged myocardial ischemia.
Background:The neuroinflammation triggered by acute cerebral ischemia can be mediated through inflammasome such as NLRP3 (NOD-like receptor family, pyrin domain containing 3) and ASC (apoptosis-associated speck-like protein). Stroke, Volume 56, Issue Suppl_1 , Page AWP399-AWP399, February 1, 2025. 17/Icr-Jcl mice in this experiment.
Advances in cardiovascular imaging have improved the ability to identify coronary artery stenosis in patients with KD, yet knowledge gaps remain regarding optimal frequency of serial imaging and the best imaging modality to identify those at risk for inducible myocardial ischemia.
For this study, acute symptomatic was defined as hemispheric ischemic stroke or retinal ischemia ipsilateral to the carotid stenosis, with symptom onset within 24 hours of admission. After adjusting for confounders, only LDL-C levels were associated with the acute symptomatic status of carotid stenosis. were asymptomatic and 40.2%
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave.
Publication date: 15 March 2024 Source: The American Journal of Cardiology, Volume 215 Author(s): Claudia Algaze, Henry Chubb, Anna M. Deitch, Thomas Collins
Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Subendocardial ischemia results in ST depression, but unfortunately, and rather mysteriously, it does not localize to the ischemic wall. Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
The precordial STD persists in severity from V4-V6, rather than being maximal in V1-V4 (as in posterior OMI), and so the ECG overall best fits the subendocardial ischemia pattern (diffuse supply/demand mismatch). Meyers serves as a reminder of the important clinical entity known as diffuse subendocardial ischemia.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
Angiography : LMCA — 90-99% osteal stenosis. LCx — 50-69% stenosis of the 1st marginal branch; with 100% distal LCx occlusion. There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. (
It should be known that each category can easily manifest the generic subendocardial ischemia pattern. In general, subendocardial ischemia is a consequence of global supply-demand mismatch that usually ameliorates upon addressing, and mitigating, the underlying cause. What’s interesting is that the ECG can only detect ischemia.
Coronary angiography gives a visual impression about the severity of the stenosis. But it need not imply the actual functional significance of the stenosis in terms of flow physiology. indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. identified physiologically significant stenosis.
Objective:To compare the 1-month stroke, myocardial infarction (MI), and/or death rates among symptomatic patients undergoing either CAS or CEA according to the timing of the procedure in Carotid Revascularization Endarterectomy versus Stenting Trial (CREST).Methods:We
The CAD Staging System is a noninvasive imaging-based investigational software device that analyzes important and actionable features of coronary atherosclerosis, stenosis and ischemia. Food and Drug Administration ( FDA ) for its Coronary Artery Disease ( CAD ) Staging System.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD. TIMI-0 flow.
This suggests further severe ischemia. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram.
Comparison Summary: ANTEROLATERAL ST CHANGES ARE NOW MORE PRONOUNCED, RATE DEPENDENT VS ISCHEMIC CHANGES Here is the Queen's diagnosis: The cath lab was activated: Culprit Lesion (s): Thrombotic 99% mid LAD stenosis with TIMI II flow Peak troponin not measured, unfortunately. So we don't have a good idea how large the final infarct size was.
His response: “subendocardial ischemia. History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. Anything more on history?
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. = This proves effective treatment of the recurrent ischemia." Here was her final EKG prior to discharge.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
Angiogram around 9am: Culprit lesion mid LAD 100% stenosis TIMI 0 TIMI 3 after PCI Severe apical dyskinesis, severe anteroapical akinesis. Instead, pain is numbed and thus ischemia is obscured with opioids, excuses like hypertension are blamed, and unnecessary CT pulmonary angiograms are focused on. None further were ordered.
of enrolled patients had critical limb ischemia, 90% had calcified lesions (30.7% stenosis in the target lesion. At baseline, 12.5% severe calcification), and there was an average of 85.5% The primary endpoint, major adverse events (MAE) at 12 months, was met with a 3.5%
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3. The peak troponin I was 0.364 ng/ml.
Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. Data from stress testing proves that the ST depression of ischemia does not localize. Culprit, stented) 3.
Transcatheter aortic valve replacement (TAVR) is increasing in popularity for symptomatic severe aortic stenosis. Absence of brachiocephalic artery occlusion which will increase the risk of intraprocedural cerebral ischemia 3. No calcifications in the artery causing vascular stenosis.
In the geometry, the size of the plaque, its relationship to luminal stenosis, arterial remodeling and eccentricity can be evaluated. Transient ischemia may occur while negotiating tight stenosis or small vessels. Plaque morphology assessment with IVUS Plaque morphology can be assessed in terms of its geometry and echogenicity.
Background Untreated multivessel disease (MVD) in acute myocardial infarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. The immediate non-IRA PCI is associated with a significantly lower occurrence of unplanned ischemia-driven PCI (OR 0.60; confidence interval [CI] 0.44–0.83)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content