This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
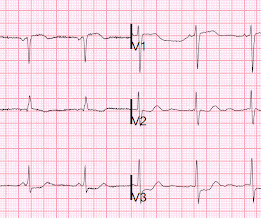
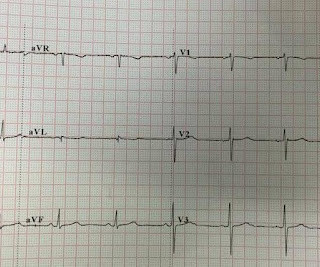
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
He interprets here: "This EKG is diagnostic of right bundle branch block and transmural ischemia of the anterior wall, most likely from an occlusion of the proximal LAD. There was a 100% proximal LAD occlusion that was opened and stented. It was recorded at 0530: What do you think? The young ED tech immediately suspected LAD OMI.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Two stents were placed with resultant TIMI 3 flow. What do you think?
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). Two stents were placed. ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. The ECG normalized overnight. Maximum troponin was 2.1
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. What do you think?
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." They found 100% acute mid-LAD Occlusion MI, stented with excellent angiographic result. Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. mm of the "required" 1.0
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. For national registry purposes, this will be incorrectly classified as a STEMI.) < 0.049).
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia.
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). ECG Blog #185 — Reviews the P s, Q s, 3 R Approach to Rhythm Interpretation.
I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. What would I expect the angiogram to show? Jesse McLaren et al.
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. It does not meet STEMI criteria. Subendocardial ischemia does not localize.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below).
This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. Right sided ECGs are best recorded in the context of inferior STEMI. Because of precordial ST depression, clinicians were also worried about posterior STEMI. This is her ECG 1.5
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls.
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH? The criteria of Armstrong et al. References 1.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Cath days later showed complete occlusion of the LAD, stented. Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! Normal vitals.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. Alternatively, it is a variant of diffuse subendocardial ischemia, with STE in V1 reciprocal to ST depression in inferior and lateral leads.
Just as hyperacute T-waves can be reciprocal to T-wave inversion ( last case ),T-wave inversion can be reciprocal to STEMI of opposite wall! Answer : There is very abnormal T-wave inversion in aVL which is typical of subtle transmural/subepicardial (due to occlusion) ischemia to the inferior wall. An 80% thrombotic RCA was stented.
Thus, there are some suspicious abnormalities, but no definite signs of ischemia. Because of persistent symptoms, another ECG was recorded 30 minutes later: There is only one new finding on this ECG which suggests ischemia. The difference is significant and highly suggests posterior ischemia. It is very subtle but real.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. It was stented. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5, There was good flow.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Lessons: 1.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." New ST elevation diagnostic of STEMI [equation value = 25.3 It was stented. Computerized QTc = 417.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. It was opened and stented. Therefore it is not a STEMI. Some are STEMI-equivalents. RCA: dominant.
He underwent coronary stenting (uncertain which artery). Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chest pain are nearly diagnostic of ischemia. Ischemia on the ECG can be very subtle and is easily missed. Lesson : 1.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So the RCA was stented. Vitals were HR 58 BP 167/70 R20 sat 96%.
One stent was deployed with restorative TIMI-0 flow. link] deWinter first reported his unique characteristics of LAD occlusion in 2008, and since the respective ECG changes do not fit the conventional STEMI paradigm (as he even stated – “instead of signature ST-segment elevation” ….) it has been subsequently deemed a STEMI-equivalent.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
More Smith comment: it is true that ST depression (STD) due to subendocardial ischemia does not localize [it is usually diffuse ST depression, in multiple leads and not reciprocal to ST elevation in an opposite territory], this ST depression is different! Both were stented. Subsequent echo showed no wall motion abnormality.
Normal RBBB, no evidence of ischemia. It was opened and stented. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct. Most STEMI peak at over 10 ng/mL; most NonSTEMI at less than 10 ng/mL. Here is the patient's previous ECG (Figure 2): Previous ECG.
It could at least say: "ST Elevation, consistent with normal variant," or "consistent with ischemia or normal variant," or "consistent with early repolarization." So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. mm in men over age 40.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content