This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse McLaren illustrates the paradigm shift from STEMI to Occlusion MI (OMI) through 9 cases, and drives home the points that if there is STEMI criteria, consider false positives (eg. secondary and proportional to LVH or BER); if there is no STEMI criteria, consider false negatives and look for other signs of occlusion (eg.
Does the ECG represent STEMI-negative OMI findings? ischemia) or it can be secondary to abnormal depolarization (e.g Discussion: The ECG in today's case does not have typical ST depression vector of diffuse subendocardial ischemia. ST depression has a variety of different causes other than ischemia.
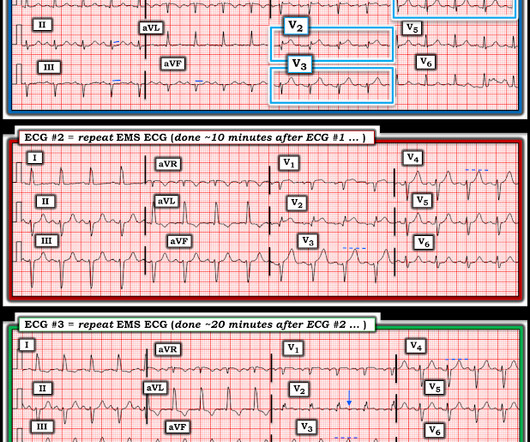
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. This confirms that the pain was ischemia and is now resovled. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He was given aspirin and sublingual nitro and the pain resolved.
Cath lab declined as it is not a STEMI." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! It is a mass delusion.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
The admission and discharge diagnosis both attributed the ECG changes and echo findings to ischemia. The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. baseline ECGs may fluctuate over time, and not necessarily represent dynamic ischemia 4.
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. Do you need posterior leads?
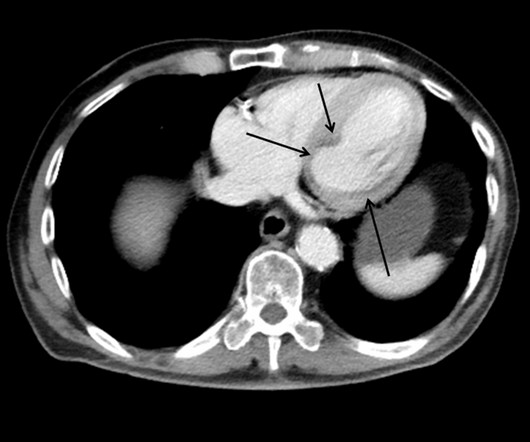
This case shows a CT image of subendocardial ischemia. However, there are also Q-waves inferiorly and the inferior T-waves are inverted, suggesting that this is an old MI with persistent ST elevation, or, alternatively, a subacute or partially reperfused, inferior STEMI. This is all but diagnostic of inferior-posterior STEMI.
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
There may be ischemia present, but it is not evident on the ECG. LVH and the diagnosis of STEMI - how should we apply the current guidelines? This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. How about diagnosing anterior STEMI in the setting of LVH? All troponins were negative.
This study shows that for a transient STEMI ("complete normalization of ST segments"), it is not unequivocally necessary to activate the cath lab emergently. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded. See more cases of Transient STEMI here: [link]
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Cardiac arrest #3: ST depression, Is it STEMI? And what do you want to do?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Figure-4: ECG findings to look for when your patient with new-onset cardiac symptoms does not manifest STEMI-criteria ST elevation on ECG. This blog post reviews the basics for predicting the " C ulprit" A rtery ( as well as reviewing why the term "STEMI" — should replaced by " OMI" = O cclusion-based MI ). Smith’s ECG Blog.
And guess what.they all show acute ischemia! The post ECG Cases 1: Missed Ischemia – Never Trust the ECG Computer Interpretation appeared first on Emergency Medicine Cases.
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. There is about 1 mm of STE in aVR I con sidered but rejected subendocardial ischemia. Is it subendocardial ischemia, or inferior MI? Here is his prehospital ECG: Diagnosis?
This ECG is diagnostic of anterior STEMI. This is likely because 1) the ischemia to the inferior wall was only partial and 2) it reperfused quickly. The QRS is at least as important as the ST segment in diagnosing STEMI It has been constant since then. He looked ill and diaphoretic. BP was 160. Lessons: 1.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Instead we discussed 5 minute delays for the STEMI(+) OMI patients.
See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. Both support acute anterior STEMI. After the hyperacute phase, the ST segments rise and only fall with either 1) reperfusion or 2) prolonged ischemia leading to irreversible infarction.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. This rules out subendocardial ischemia and is diagnostic of posterior OMI. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
There is no ST depression in V6, II, III, or aVF, and no significant ST elevation in aVR, all confirming that the ST vector is not consistent with diffuse subendocardial ischemia, but rather a focal ST vector pointed at the posterior wall. Obvious inferoposterior STEMI. It is posterior OMI until proven otherwise.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
This was a machine read STEMI positive OMI. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chest pain. His ECG is shown below.
911 was called and the medics recorded this ECG (unfortunately, leads V4-V6 are missing) Due to marked ST Elevation, the computer read was STEMI What do you think? A 20-something male drank heavily of ethanol and used cocaine, then was involved in a stressful verbal altercation, at which time he developed chest pain.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. What do you think?
ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. ECG Blog #230 — Reviews HOW to c ompare S erial E CGs ( ie, "Are you comparing Apples with Apples or Oranges?" ).
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. A posterior ECG was done and showed no ST elevation, not even 0.5 The ECG normalized overnight.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
Instead, pain is numbed and thus ischemia is obscured with opioids, excuses like hypertension are blamed, and unnecessary CT pulmonary angiograms are focused on. This patient does not show up in the STEMI registry, and the time to reperfusion will likely not be identified as the problem that it was.
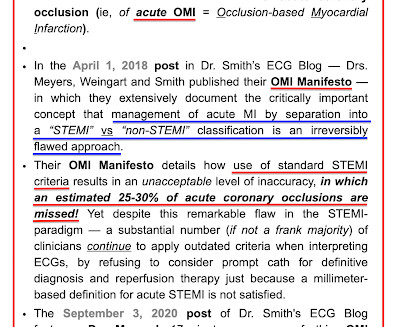
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. A millimeter definition of acute STEMI should not be needed to justify the need for prompt cardiac catheterization.
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
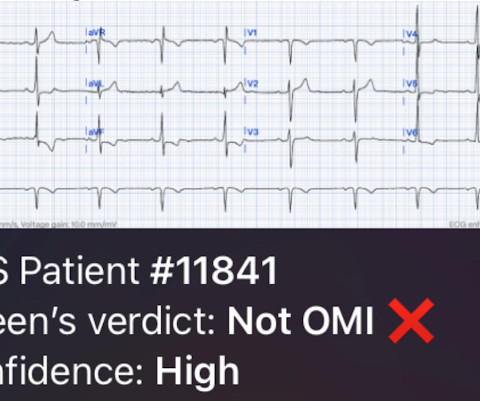
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
ST depression in the setting of acute transmural ischemia (STEMI) is almost ALWAYS due to reciprocal change. The elevation is higher in Lead III than in Lead II, a reliable sign of RCA occlusion. Reciprocal depression in Leads aVL and I. Reciprocal depression in V1 - V3.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content