This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
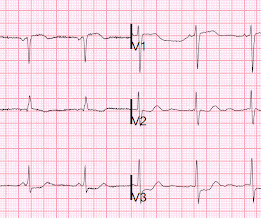
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
Xray was consistent with pulmonary vascular congestion. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely.
There was some pulmonary edema. This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. Perusal of her charts revealed that she had an LAD stent that was very close to the ostium of the circumflex. AT&T surprised me with their reach. This is her ECG 1.5
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. A majority of patients with MAT have longstanding pulmonary disease. No significant changes, ongoing pain.
Outcome In the EVAR group, 47 patients (95.92%) were successfully implanted with overlapping stents, and 2 patients died in the perioperative period. In the TAAR group, 12 patients (92.31%) were successfully revascularized and 1 patient died in the perioperative period.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. This was stented. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. He appeared to be in shock.
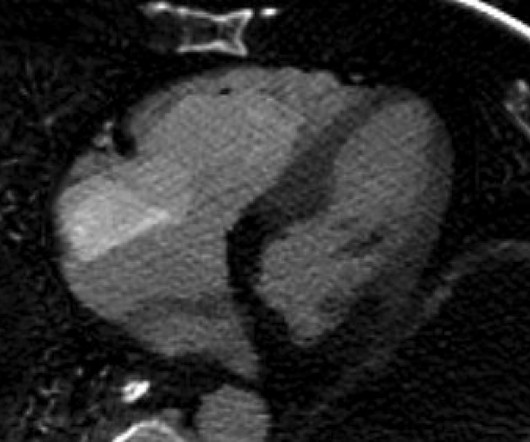
It did not show pulmonary embolism or intra-abdominal pathology, but it did show this: See the dark area at the bottom of the image? There is Transmural ischemia of Occlusion MI. Spectral CT This spectral CT image really highlights the dense transmural ischemia of the posterior wall. There was no pulmonary embolism.
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Also: electrical instability, pulmonary edema, or hypotension. Another EKG was also obtained.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content