This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Does the ECG represent STEMI-negative OMI findings? ischemia) or it can be secondary to abnormal depolarization (e.g Discussion: The ECG in today's case does not have typical ST depression vector of diffuse subendocardial ischemia. ST depression has a variety of different causes other than ischemia.
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible. Smith SW.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. This rules out subendocardial ischemia and is diagnostic of posterior OMI. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
Xray was consistent with pulmonary vascular congestion. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely.
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. To me, this looks like pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. Here are a few clips.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. Look at the aortic outflow tract. What do you see?
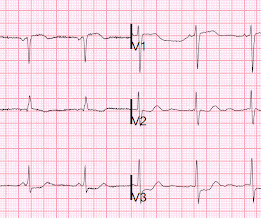
There is normal R-wave progression in the precordial leads with no evidence of ischemia. large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. Any cause of pulmonary hypertension. What do you think?
There was some pulmonary edema. This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. Right sided ECGs are best recorded in the context of inferior STEMI. Because of precordial ST depression, clinicians were also worried about posterior STEMI.
Is this an anterior STEMI with LBBB? Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. Additionally, appropriate discordance is common in NonSTEMI, but very unusual in coronary occlusion (STEMI).
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
I knew that, if the patient had presented with chest discomfort, that this ECG is diagnostic of inferior posterior OMI, even though it is not a STEMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
Was there pulmonary edema? Repeat ECG showing no STEMI, only non-specific ST-segment and T-wave abnormalities, unchanged from prior" Transferred to surgery for exploration but diagnostic studies were too indeterminate to be certain of intra-abdominal pathology. Then they were worried about sepsis as an etiology of hypotension.
It does not usually represent subendocardial ischemia, but rather it is usually reciprocal ST depression, reciprocal to inferior ST elevation. Still does not meet STEMI criteria, but it is an obvious OMI And then another one became more obvious: Cath lab was activated and a 100% RCA occlusion was found.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. A majority of patients with MAT have longstanding pulmonary disease. Rather than antiarrhythmic medication — optimizing pulmonary function is the best treatment approach. No significant changes, ongoing pain.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 Learning Points: 1.
CT pulmonary angiogram (unnecessary, often done while missing OMI) was unremarkable. Instead, pain is numbed and thus ischemia is obscured with opioids, excuses like hypertension are blamed, and unnecessary CT pulmonary angiograms are focused on. Which is true. No repeat ECG was done at this time.
There is ST depression beyond the end of the wide QRS in I, II, aVF, and V4-V6, diagnostic of with subendocardial ischemia. It makes pulmonary embolism (PE) very likely. The small LV implies very low LV filling pressures, which implies low pulmonary venous pressure. LV anterior STEMI does not give maximal ST elevation in V1.
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. Then there is the significant ST elevation we see in lead V1.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits.
and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. CT angiogram chest: no aortic dissection or pulmonary embolism. 24 yo woman with chest pain: Is this STEMI?
I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Anything that causes pulmonary edema: poor LV function, fluid overload, previous heart failure (HFrEF or HFpEF), valvular disease. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Management?
No acute infectious prodrome, known pulmonary disease, or recent trauma. The Queen of Hearts Diagnosed "STEMI/STEMI equivalent" on that first ECG (she now uses "STEMI Equivalent" rather than OMI). No prior similar symptoms or known CAD. PMHX significant for hypertension and BPH. This is the new version of the Queen.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Also: electrical instability, pulmonary edema, or hypotension. Another EKG was also obtained.
Bedside POCUS showed very poor LV function and a few pulmonary B lines. A Chest X-ray did not show pulmonary edema. Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved. He was put on BiPAP. Next day, with K = 4.6
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. she had severe pulmonary edema. She was BVM ventilated and suctioned. From this site.
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. See Raitt et al.:
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content