This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
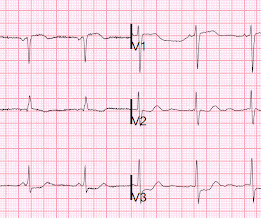
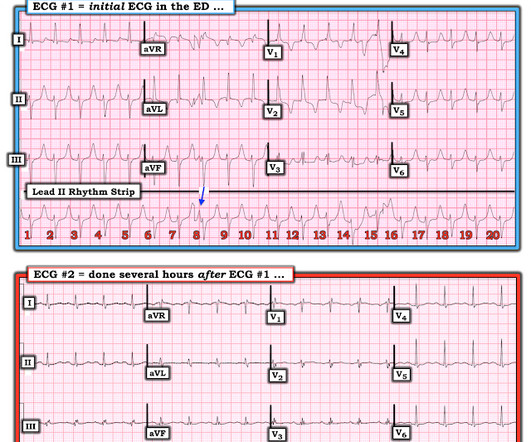
That said — the ECG in Figure-1 should prompt the following considerations: The symmetric chest lead T wave inversion in ECG #1 could be a sign of coronary disease, potentially with acute ischemia. Stat Pulmonary CT angiography was ordered — and confirmed acute PE. P.S. = PEARL # 3: An Often Forgotten Clinical NOTE.
ischemia) or it can be secondary to abnormal depolarization (e.g Discussion: The ECG in today's case does not have typical ST depression vector of diffuse subendocardial ischemia. The ST vector in subendocardial ischemia (SEI) usually has the largest amount of ST depression in leads II and V5, towards the apex of the heart. (ST
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. million patients in the United States.
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. The CXR demonstrated no pulmonary edema. Type I ischemia.
The therapeutic effect, total myocardial ischemic burden (TIB), the effective rate of TIB reduction, pulmonary function indices, cardiac function, and the incidence of adverse events compared between the two groups.ResultsThe intervention group demonstrated a higher effective rate.
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
There is also STE in lead III with reciprocal depression in aVL and I, as well as some subendocardial ischemia pattern with STD in V5-V6 and STE in aVR. Aslanger's is a combination of acute inferior OMI plus subendocardial ischemia, and due to the ischemia vectors , it has STE only in lead III. Moreover, there is tachycardia.
Xray was consistent with pulmonary vascular congestion. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely.
The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
This middle-aged patient presented with SOB, weakness, and mild pulmonary edema. There was no evidence of ischemia. In addition to ruling out rate-slowing medication serum electrolyte disorders and/or ischemia/infarction as potential causes of bradyarrhythmias one should also rule out hypothyroidism + sleep apnea.
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. To me, this looks like pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. Here are a few clips.
There is normal R-wave progression in the precordial leads with no evidence of ischemia. large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. Any cause of pulmonary hypertension. What do you think?
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. She was intubated.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentr y tachycardias — atrial fibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction.
Transcript of the video: Eisenmenger syndrome is an important complication of large left to right shunts which develop later due to development of pulmonary vascular obstructive disease and severe pulmonary hypertension. So in ASD Eisemenger, suprasystemic pulmonary hypertension is possible. But, leave that alone.
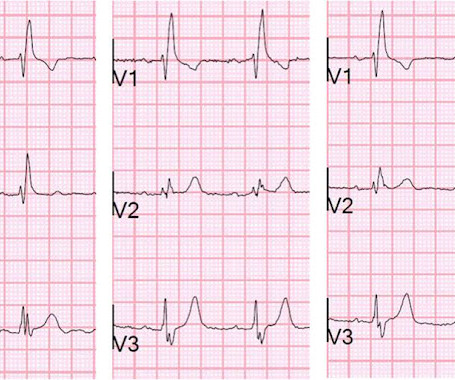
After resolution, there was T-wave inversion in V1-V3, highly suggestive of ischemia. There are features of the T-wave inversion, however, which argue against ischemia. Also, anterior ischemia is unlikely to spare lead V4 as in this case. This phenomenon is poorly understood, but involves "transient electrical remodeling."
There was some pulmonary edema. This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. They texted me the following ECGs, which I viewed in the shade of a pine tree on a glorious sunny snowy landscape. AT&T surprised me with their reach.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different. Here are V1-V3 from the last 3 ECGs: It is now clear that there is cardiac ischemia. 56 y/o male who presented with 12/10 severe chest pain starting at 3AM, radiating to his upper back. Wraparound? It was negative.
Ischemia assays were used to examine the cell capacity for vascular malformation. This new population was referred to as arterial-lymphatic-like ECs according to its cellular markers, and its appearance was validated in the pulmonary small arteries afterAlk1deletion. Transplantation of these cells caused vascular malformations.
remain hypo- or akinetic for some time even if not infarcted, just due to the profound ischemia incurred during the occlusive phase. Thus, an acute wall motion abnormality is not a sign of active or persistent ischemia, and thus is not necessarily an indication for emergent cath. Even many NOMI have wall motion abnormalities.
Advanced cardiac imaging especially in atypical presentations, can aid in early diagnosis.Case:A 59 year-old man with history of biopsy-proven pulmonary sarcoidosis presented with non exertional chest pain for 2 months. Stress echocardiogram ruled out myocardial ischemia.
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. Obviously he has multiple reasons to have pulmonary hypertension.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Q waves in association with RBBB are usually not seen in anterior leads unless there is pulmonary hypertension or anterior infarction. Chest trauma was suspected on initial exam.
Low LV filling pressures are due to several etiologies, most commonly due to volume depletion (dehydration or hemorrhage), but also due to other etiologies including, but not limited to: mitral stenosis, pulmonary hypertension (chronic, or due to pulmonary embolism), or poor RV performance.
A subset of NSTEMI precipitated by acute severe HT and flash pulmonary edema has excellent prognosis if BP is reduced promptly. Global ST depression (AVR.V1 might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset Onset of NSTEMI-CS occurs late (48-72 hrs) 3.Severe
Clinical evaluation and X-Ray chest showed features of pulmonary edema. ST segment elevation in aVR in proximal LAD occlusion before first septal is thought to be due to transmural ischemia of the basal part of the septum. ST segment elevation is noted in aVR.
It does not usually represent subendocardial ischemia, but rather it is usually reciprocal ST depression, reciprocal to inferior ST elevation. There are many potential causes of ST-T wave abnormalities (ie, LV “strain” from LVH; medication effect; electrolyte disturbance; pulmonary embolus, etc.). Sounds like reflux, right?
hours ECG: Not much change hs troponin I peaks at 500 ng/L 8 hours Next morning Urine drug screen: Amphetamine, Methamphetamine, Fentanyl, Fentanyl metabolite Formal Bubble Contrast Echocardiogram: Indications for Study: Silent Ischemia. The estimated pulmonary artery systolic pressure is 29 mmHg + RA pressure.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. A majority of patients with MAT have longstanding pulmonary disease. Rather than antiarrhythmic medication — optimizing pulmonary function is the best treatment approach. No significant changes, ongoing pain.
Was there pulmonary edema? Furthermore, there are T-wave changes in V2 and V3 which are highly suggestive of ischemia, but difficult to localize: anterior? Then they were worried about sepsis as an etiology of hypotension. Then the notes mention "cardiogenic shock" but without any reference to a cardiac echo or to a chest x-ray.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
He was seen at another hospital and found to have a slightly elevated troponin, then underwent a CT pulmonary angiogram (PE) protocol which revealed a right sided pneumonia. The septum appears a bit darker than the rest, and you might be fooled into thinking there is ongoing ischemia here. See an examples of CT ischemia here.
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. The estimated pulmonary artery systolic pressure is 37 mmHg + RA pressure. Normal estimated left ventricular ejection fraction lower limits of normal.
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentr y tachycardias — atrial fibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction.
Either could be a result of myocardial contusion There is some minimal ST depression -- this could represent ischemia What else is there that could use therapy immediately? The estimated pulmonary artery systolic pressure is 49 mmHg + RA pressure. There is a very long ST segment resulting in a very long QT.
Up to 50% of patients with pulmonary embolism (PE) experience hemodynamic instability and approximately 70% of patients who die of PE experience an accelerated cascade of symptoms within the first hours of onset of symptoms, thus necessitating rapid evaluation and intervention. Journal of the American Heart Association, Ahead of Print.
In this case, the patient was not in extremis (he was awake, without pulmonary edema or cardiac ischemia), so we could proceed to treat it in stepwise fashion with fluids, then cardioversion, then pericardiocentesis. Fluids may help, but restoring sinus rhythm is even more important. Each step improved the patient's condition.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
Source: JAMA Cardiology) Patients with afib who survived an intracerebral haemorrhage had a very significant risk of cerebrovascular ischemia episodes and death in the following year, according to registry data. JACC: Asia) Lexaria Bioscience has announced that a CBD product beats a placebo in simulating acute pulmonary hypertension.
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. Then there is the significant ST elevation we see in lead V1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content