This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This EKG is diagnostic of transmural ischemia of the inferior wall. The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Lead I also shows reciprocal ST depression.
This suggests further severe ischemia. MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. And yet the arteries remain open.
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable riskfactors for coronary artery disease. This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. I performed bedside echocardiography.
Given the consistency of the clinical profile with typical angina, associated riskfactors, and abnormal ECG findings, a cardiology consult was promptly requested. It should be known that each category can easily manifest the generic subendocardial ischemia pattern. What’s interesting is that the ECG can only detect ischemia.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
No thromboembolism risks, not pleuritic, no radiation to the back. No cardiac riskfactors, no cocaine use. T-wave inversion in V2 is inconsistent with early repol, and is typical of posterior ischemia. In addition, there is ST depression, diagnostic of ischemia, in V3-V6. History: Onset of CP 2.5
She had zero CAD riskfactors. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. hours of substernal chest pressure.
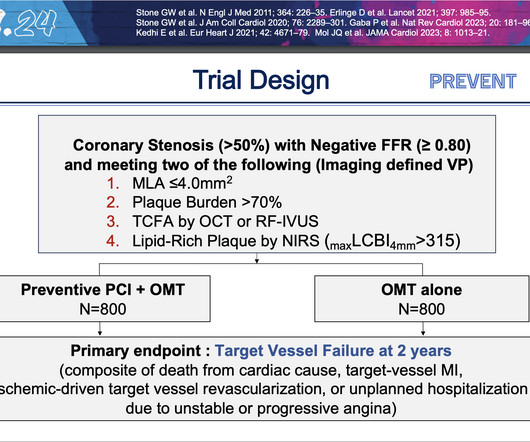
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood. These findings demonstrate that the focal treatment of high-risk vulnerable plaques may improve patient prognosis beyond optimal medical therapy alone.”
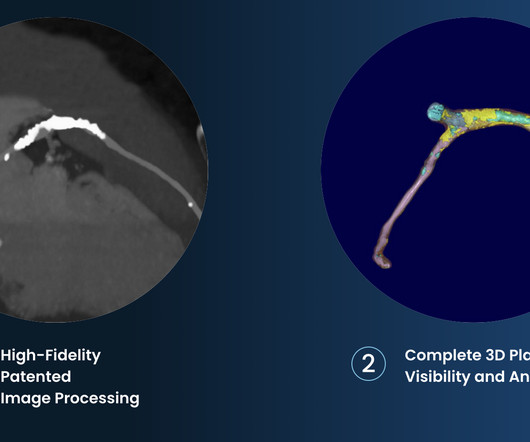
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. Márton Kolossváry (Gottsegen National Cardiovascular Center, Budapest, Hungary).
Implementation of a multispecialty care team approach, including expertise in riskfactor management, guideline directed medical therapies, wound and foot care and endovascular and surgical revascularization procedures, may improve outcomes for people with PAD. . and Global Data From the American Heart Association.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardial infarction (MI), stroke, and cardiovascular (CV) death.4
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. There are 3 types of coronary atherosclerosis visible on CTCA: Calcified Plaque - Easily Identified on both CT CAC & CTCA scans. Subscribe now How Often Does A CT CAC Scan Miss Plaque?
(Naturopathic Medicine) According to a subanalysis of a randomised study, low-dose edoxaban (Savaysa) was related with a reduced stroke risk and a negligible increase in bleeding in older Afib patients at high bleeding risk.
Introduction:Stroke is a well-established independent riskfactor for the development of dementia. Most dementia patients exhibit mixed brain pathologies, with histological evidence of ischemia and A plaque accumulation, observed at autopsy.
Arteries generally narrow and occlude for one of two reasons: The progressive accumulation of plaque. A plaque ruptures, and a clot forms in the artery, thereby occluding it. There are the ‘garden variety’ heart attacks whereby a plaque ruptures in the coronary artery, called a spontaneous heart attack. N Engl J Med.
Smith Major Learning Point: The worst riskfactor for a bad outcome in OMI is young age because cardiologists cannot believe that a young person can have an OMI. Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. This gets drilled into them.
In this case, the context is a 51 year old man with riskfactors presenting with acute onset substernal chest pain with nausea and vomiting. The operator performed intravascular ultrasound and visualized acute plaque rupture with thrombus formation and placed a stent. The pre-EKG probability for OMI could hardly be much higher!
Like, viability, scars, futility, and benefits of revascularization, imaging-assisted PCI, impact of PCI on exercise capacity, importance of riskfactor management, etc. He was so knowledgeable and was aware of everything I wanted to tell. What is the big deal to analyze suboptimal PCI vs OMT? 2016 Dec;9(12):e003726.
Still, an ECG was obtained at 0649hrs: (Digitized by PM Cardio) McLaren: The patient has a high pretest probability based on age, riskfactors and symptoms. Influenza-like illness can also trigger plaque rupture. The posterior lead V9 is clearly misplaced, as it should be relatively reciprocal (opposite) in morphology to V2.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content