This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
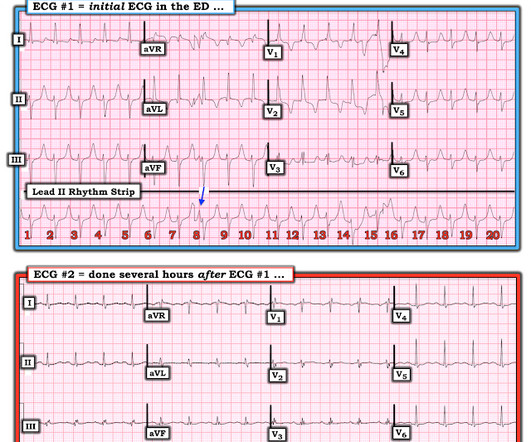
The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits.
And superimposed subendocardial ischemia pattern, of course. Smith's ECG Blog — the presence of an almost “null vector” in standard lead I ( ie, P wave, QRS complex and T wave all under 2mm in size ) — is highly suggestive of longstanding and severe pulmonary disease. She was otherwise very stable during this rhythm.
Either could be a result of myocardial contusion There is some minimal ST depression -- this could represent ischemia What else is there that could use therapy immediately? The estimated pulmonary artery systolic pressure is 49 mmHg + RA pressure. There is a very long ST segment resulting in a very long QT.
Evidence of acute ischemia (may be subtle) vii. Of the 67 patients who underwent targeted tests, suspected diagnoses were confirmed in 49 (73%) patients: aortic stenosis (n = 8, 1%), pulmonary embolism (n = 8, 1%), seizures/stroke (n = 30, 5%), and other diseases (n = 3). Left BBB vi. Pathologic Q-waves viii. LVH or RV d.
For right or wrong reasons, the world of electrophysiology has pushed us into a belief system that, if it is AF, the culprit must be pulmonary veins. In fact, non-pulmonary vein origins can be a staggering 70% in some series. Only 20% of focal AT arise from pulmonary veins. I guess, the same should be true for AF. Reference 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content