This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This groundbreaking study, delving into the physiological intricacies during exercise, specifically targets patients with ANOCA and MBs, utilizing wave intensity analysis. 2023 The post Decoding the Menace Within: Unraveling Myocardial Bridges and Exercise-Induced Ischemia appeared first on Cardiology Update. Circ Cardiovasc Interv.
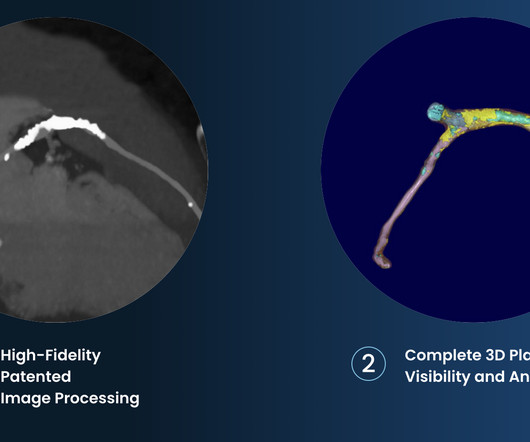
Food and Drug Administration ( FDA )-cleared Cleerly ISCHEMIA software device applied to a non-invasive coronary CT angiogram ( CCTA ) can be billed using the new Category I CPT code 75580. Prior studies have demonstrated the independent and incremental benefit of Cleerly ISCHEMIA applied to CCTA beyond traditional assessment.
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
Together, the two companies will work to further the development and commercialization of Medis Quantitative Flow Ratio (Medis QFR), a non-invasive approach to the assessment of coronary physiology, as part of GE HealthCare’s interventional cardiology portfolio built around the Allia Platform.
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Diagnosis and treatment of ischemia-producing coronary stenoses improves 5-year survival of patients undergoing major vascular surgery.” 2024, [link].
LSCI demonstrated a 2-to-5-fold increase in the area of profound ischemia (lowest quintile of pixel values) in the Koizumi model compared to the Longa model and with increasing ischemic duration.
Background:Malonate, a competitive inhibitor of succinate dehydrogenase, has shown much promise in ameliorating ischemia/reperfusion injury (IRI) in various diseases, including ischemic stroke. Stroke, Volume 55, Issue Suppl_1 , Page AWMP12-AWMP12, February 1, 2024. or low pH (6.0).
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
The company is also pursuing an indication for non-invasive measurement of fractional flow reserve (FFR CT ), uniquely derived from its plaque algorithm, to measure coronary blockages and the extent of ischemia.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
BackgroundAcute psychological stress may induce physiological changes predisposing individuals to adverse health outcomes through hemodynamic and vascular effects. Journal of the American Heart Association, Ahead of Print.
Endothelial cell (EC) sensing of elevated fluid shear stress (FSS) from blood flow induces vessel outward remodeling to restore physiological FSS, but mechanisms are poorly understood. In a mouse arteriovenous fistula (AVF) model, high FSS induces arterial outward remodeling coincident with elevated BMPER expression and Smad1/5 inactivation.
mm in diameter, 3 mm in length) containing zirconium dioxide was advanced in the catheter by injection of physiological saline to establish local occlusion. A blood clot (0.86 Both fluoroscopy at 1, 3, 6, 24 h and TTC staining at 24 h after stroke model creation were performed.
We have also shown several cases in which atrial flutter hides true, active ischemia. Likewise, in some cases of ischemia concealed by flutter waves, the ischemia can be seen despite the flutter waves, whereas in other cases the dysrhythmia must be terminated before the ischemia can be clearly distinguished.
Intro:Resources for studying stroke are limited to clinical trials with sparse access to physiological and biochemical details, and pre-clinical animal studies with limited relation to humans. A physiologically accurate in silico model would provide a new route for study of the response to an ischemic event.
Historical and ongoing research acknowledges the endocannabinoid system's crucial role in managing physiological processes, suggesting cannabinoids could offer therapeutic benefits in post-surgical recovery.
Computational models of cerebrovascular ischemia are well-suited to such exploration, and the use of digital phantoms for sophisticated biophysical modeling has been facilitated by emergent hardware, software, and computational solutions.
But it need not imply the actual functional significance of the stenosis in terms of flow physiology. indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. There is a strong correlation between FFR and inducible myocardial ischemia. identified physiologically significant stenosis.
Serial echo monitoring showed increasing pericardial pressures without overt tamponade physiology. That said — I did not interpret these differences as the result of acute ischemia. Echo showed a new large pericardial effusion with large focal hematoma in the posterior pericardium near the descending thoracic aorta/TEVAR edge.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits. These include.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) The atrial rate is around 120 beats per minute, which indicates high adrenergic state and physiologic distress! I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ).
This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2] Chapter 6: Introduction to Myocardial Ischemia and Infarction. Physiology. 2] Birnbaum, Y., 3] Costanzo, L.
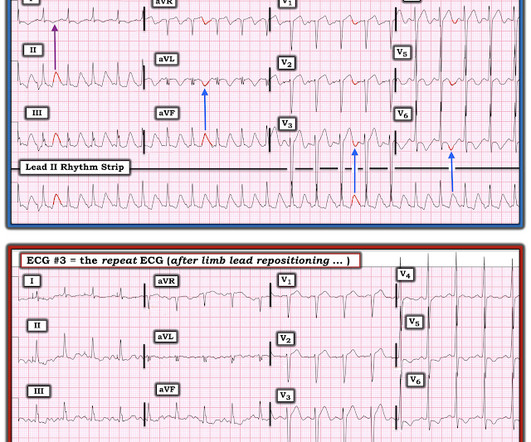
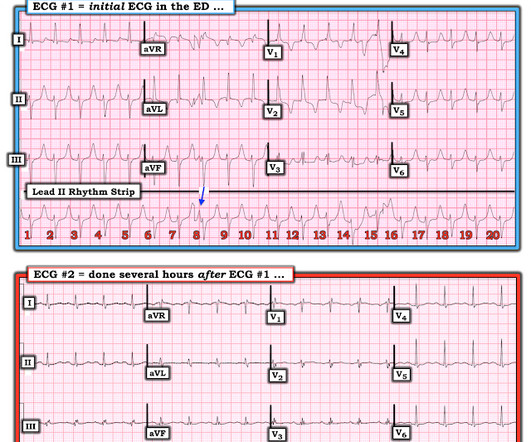
The ECG was incorrectly interpreted as no signs of ischemia. Artificial intelligence can be trained to recognize subtle OMI = My Comment by K EN G RAUER, MD ( 2/6 /2023 ): = The initial ECG in today's case was incorrectly interpreted as, "No signs of ischemia". Figure-1: Comparison of the first 3 ECGs in today's case.
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. The QRS complex in ECG #1 is wide.
And superimposed subendocardial ischemia pattern, of course. It simply does not make physiologic sense to suddenly see an all-negative QRS complex in this most lateral chest lead. Several minutes later there was a change in the monitor, and she reported increased palpitations: With the context, this is almost certainly 1:1 flutter.
2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia. 3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4]
Neuroadaptation after chronic cocaine use is less well understood though rat models suggest that as cerebral ischemia develops from chronic cocaine use, the HIF‐VEGF pathway is activated to promote angiogenesis to restore local blood flow[3].
This transmural ischemia, but not necessarily completed infarction (yet). See more images of this case at Gopal's Spectral CT Blog: It's all about confidence With continued symptoms, an elevated troponin, and no other explanation, this is acute MI with ongoing ischemia until proven otherwise.
We wish, our understanding about cardiac contractile physiology is deep and nearly complete. The simple reason could be we can address the ischemia a potential arrhythmic target by some form of revascularization in IDCM. Heart is an irreversibly coupled electro-mechanical organ , right from the fetal days until the final heart beat.
It is also unique because it works using the Doppler effect, you can get not only an anatomical evaluation of the heart but also physiological assessment. These are therefore not looking for coronary disease but instead ischemia heart disease. It is still possible to have ischemia without coronary disease.
It is interesting to note, while plasminogen levels are elevated, D-dimer is also increased, indicating an ongoing fight between pro & anticoagulant forces, converting the physiological maternal- placental bed a mini harmless DIC equivalent zone. What does it imply ?
Pain will resolve with completed infarct or with resolution of ischemia. ECG recorded at 7 hours All active ischemia is gone. Pain will resolve not just with resolution of ischemia, but with completion of infarction. This T wave progression sequence does not make physiologic sense. This looks like infarct completion.
V2 never has this appearance in the absence of full thickness ischemia. There is a small amount of reciprocal STD in V6 with a negative T-wave. This is subtle but diagnostic for anterior Occlusion MI. We called for emergent cath lab activation. The cardiologist arrived quickly and was skeptical about these findings on EMS ECG.
I thought the dramatic increase in chest lead amplitudes ( ie, very deep S waves in anterior leads — with very tall R waves in V5,V6 ) — together with tall, peaked anterior T waves — and QTc prolongation with deep symmetric T wave inversion in V5,V6 — could all be explained by marked LVH with LV “strain” and/or ischemia.
At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention. What about the 1 2- L ead E CG ? As already established — the QRS complex is narrow in all leads, so the rhythm is supraventricular. The QTc is not overly prolonged.
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. Smith pointed out that while atropine may may result in slightly more oxygen demand, the increase in cardiac output and in blood pressure would increase overall coronary perfusion and decrease ischemia.
If you still have not read it, I strongly recommend that you read the following article on the diagnosis of "posterior" MI: Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia), by Meyers HP et al. J Am Heart Assoc. doi: 10.1161/JAHA.121.022866.
The physiologic basis for the finding of LVH on ECG, is that with increases in left ventricular mass — electrical forces directed toward the LV ( left ventricle ) increase, and this produces larger R wave amplitude in one or more left-sided leads (ie, leads I, aVL, V4,5,6 ).
Either could be a result of myocardial contusion There is some minimal ST depression -- this could represent ischemia What else is there that could use therapy immediately? Or, much less likely, it could be a very accelerated escape rhythm from the posterior fascicle. There is a very long ST segment resulting in a very long QT.
Biological sex is an important modifier of physiology and influences pathobiology in many diseases. The heart is a remarkably plastic organ and rapidly responds to physiological and pathological cues by modifying form and function. Finally, we offer a perspective on key future directions for research into cardiac sex differences.
In MSIMI (Mental Stress-induced Myocardial Ischemia) studies , mental stress activities like public speaking were evaluated for their impact on ischemia, measured via myocardial SPECT and vascular function (microvascular function, endothelial function).
Evidence of acute ischemia (may be subtle) vii. ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. Fourth, syncope in the elderly often results from polypharmacy and abnormal physiologic responses to daily events. 2nd or 3rd degree AV blocks or sinus pause of at least 2 seconds iv.
But the definite ST segment flattening and depression in leads V4 , V5 , V6 is real and given the history of new severe CP this has to be assumed as acute ischemia until proven otherwise. Physiologically this may occur as a result of very brief coronary occlusion, followed so soon after by spontaneous reperfusion.
The fact that the heart rate is normal rules out demand side ischemia as well. Interpretation of T-wave inversion in physiological and pathological conditions: Current state and future perspectives. In this case, it was taken in a 36-year-old woman, routine health check and has no specific symptom. Have seen a HCM variants like this ).TMT
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content