This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
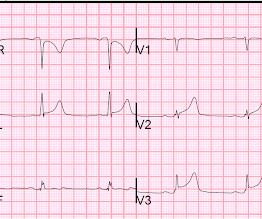
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury.
This ECG is diagnostic of anterior STEMI. But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. Add that to "sharp" pain and a 33 year old, and it is easy to convince yourself that this is, indeed, pericarditis. However, look closely! Lessons: 1.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Pericarditis maybe." There was no prior ECG for comparison.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Clinician and EKG machine read of acute pericarditis. While it is true that inferior MI has ST depression in aVL 99% of the time (Bischof and Smith), and that inferolateral ST elevation is the most common distribution for pericarditis, the ST elevation in V3 has "terminal QRS distortion (TQRSD)," (diagnostic of LAD occlusion).
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). As already mentioned, this patient could have post-infarction regional pericarditis from a large completed MI. Sinus tachycardia has many potential causes.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
More Smith comment: it is true that ST depression (STD) due to subendocardial ischemia does not localize [it is usually diffuse ST depression, in multiple leads and not reciprocal to ST elevation in an opposite territory], this ST depression is different! When there is STE in V4-V6, and in inferior leads, there is no ST depression in V2-V4.
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Weren't you taught that "new tall T wave in V1" is concerning for ischemia, and so this is the opposite?
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? Well, don't we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia.
Normal RBBB, no evidence of ischemia. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct. Patients with completed, transmural infarct are also at risk for post-infarction regional pericarditis and myocardial rupture. R-waves of of normal height.
You do NOT see this in normal variant STE, nor in pericarditis. The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI.
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. Assessment:" " Nonspecific ST elevation from V1-V4 , question of early repolarization versus pericarditis , question of acute current of injury and ? Pericarditis would be even more unlikely in someone without chest pain.
cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." It does take some time for thrombus to form, but the EKG and the troponin profile show that this was NOT a late presentation STEMI. of AMI patients and is often preceded by postinfarction regional pericarditis (PIRP).
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. 24 yo woman with chest pain: Is this STEMI? Pericarditis? Beware a negative Bedside ultrasound.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. There is also ST depression in precordial leads, greatest in V3 and V4, concerning for posterior STEMI. What was the inciting factor? The diagnosis is in doubt.
Smith : I recognize this as a STEMI mimic. Doesn't this necessarily mean that he was having ischemia? Here is his ECG: There is significant ST Elevation in inferior leads, with reciprocal ST depression in aVL. This appears to be an inferior OMI What do you think? I was not alarmed. What does the Queen of Hearts think? "No
.: 50% of LAD STEMI have Q-waves by one hour. The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves. So it is not necessarily subacute.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content