This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. For national registry purposes, this will be incorrectly classified as a STEMI.) < 0.049).
Again, see Ken's discussion below) Discussion continued The absence of pace spikes suggests this is not a pacemaker/ICD-related rhythm in this patient with an ICD. Are the apparent P-waves (which now we suspect might not be P-waves) actually part of the QRS, in which case the QRS is even wider than it appears? Where does the QRS begin?
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. It’s important to stress the presence of a normal QRS (i.e.,
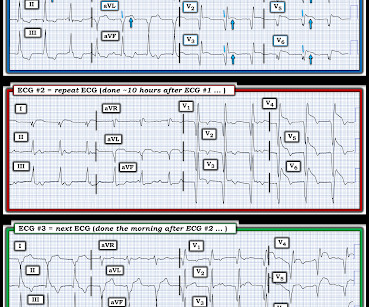
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. It is also not a wandering pacemaker — because change in atrial pacing site is gradual with that disorder. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression.
100% occluded RCA with TIMI 0 flow Post drug-eluting stent placement with TIMI 3 flow While in the cath lab, she transiently developed complete heart block and became hypotensive requiring transvenous pacemaker placement and transient pressors. The transvenous pacemaker was removed the following day and pressors were not required again.
Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI. See these similar cases: A man in his sixties with chest pain Why is there inferior ST elevation, and would you get posterior leads?
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? The patient continued having chest pain. What is the rhythm? Moffat, M.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( The below ECG was recorded.
The medics recorded the following initial ECG at time 0: The computer read (see below) gives no further comment beyond ventricular pacemaker. And, in cases like the elderly patient with new-onset chest pain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. What do you think?
PEARL # 2: Despite the challenge of assessing a ventricular rhythm for underlying ischemia and/or infarction there are primary ST-T wave changes that are seen in Figure-3 that suggest an ongoing acute event. In contrast emergency ( and/or longterm ) pacing may be needed when complete AV block is the result of acute infarction.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content