This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
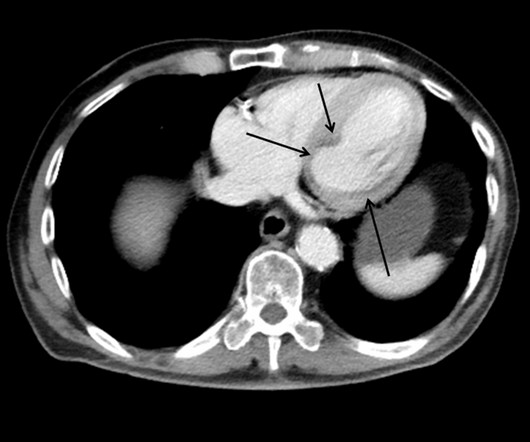
This case shows a CT image of subendocardial ischemia. However, there are also Q-waves inferiorly and the inferior T-waves are inverted, suggesting that this is an old MI with persistent ST elevation, or, alternatively, a subacute or partially reperfused, inferior STEMI. This is all but diagnostic of inferior-posterior STEMI.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits. These include.
9 However, because troponin is a clear marker of disease severity and a powerful independent predictor of adverse outcomes, it may be quite useful in the ED disposition decision: if troponin is elevated, then outpatient management should be reconsidered. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0
There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Use STEMI criteria to identify acute coronary occlusion: the ECG was STEMI negative 2. A repeat ECG was done on way to cath lab: "STEMI negative" again. The cath lab was activated. Take home 1.
Smith : I recognize this as a STEMI mimic. Doesn't this necessarily mean that he was having ischemia? But vasovagal syncope typically has a prodrome such that further evaluation of today's patient may be needed as an outpatient to better assess for the cause of his sudden syncope. I was not alarmed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content