This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Introduction The use of contemporary drug-eluting stents (DES) has significantly improved outcomes of patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI). cases, the target lesion was in-stent restenosis (ISR). At 1 year, only two (0.5%) subjects presented ischemia-driven TLR.
Smits and a distinguished team of international researchers, the trial compares the performance of SMT's biodegradable-polymer sirolimus-eluting Supraflex Cruz stent with the biodegradable-polymer Ultimaster Tansei * stent in patients with high bleeding risk (HBR) undergoing abbreviated dual antiplatelet therapy (DAPT).
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
The goal was to determine whether using FFR to identify functionally significant stenoses (FFR 0.80) for stenting, rather than relying solely on angiographic appearance. Inference Established that FFR-guided PCI is superior to angiography-guided PCI in multivessel CAD, reducing unnecessary revascularizations and improving outcomes.
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood. During PCI, an operator inserts a stent into a blocked artery through a catheter in the groin or arm.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. 4 Recent literature has reported clinical benefits associated with rescue stenting in the setting of ICAD‐related MT‐refractory strokes.5
Diseased human arteries are most simply, reliably, and successfully treated with drug-eluting, balloon-expandable stents," said Lewis B. 2 An estimated 10% of patients with PAOD have its most severe form: chronic limb-threatening ischemia (CLTI). Given this dismal outcome, the prognosis of CLTI is worse than most cancers.3,4
The Freesolve BTK RMS is designed for individuals suffering from chronic limb-threatening ischemia (CLTI). Our next generation RMS represents a leap forward over existing resorbable technology, incorporating technical innovations intended to address physicians' needs and optimize outcomes for patients suffering from CLTI.”
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
Background:Patients with atrial fibrillation were excluded from clinical trials evaluating carotid artery stent(CAS) or carotid endarterectomy (CEA).We Background:Patients with atrial fibrillation were excluded from clinical trials evaluating carotid artery stent(CAS) or carotid endarterectomy (CEA).We
Herein, we describe a single‐step approach to deploy Neuroform Atlas stent (Stryker Neurovascular, Fremont, CA) which is a hybrid laser‐cut, nitinol self‐expanding stent without the need for ELW or lesion re‐access using MINI TREK RX (Abbott Vascular, Inc., There was no restriction on time from last known well (TLKW) to MT.
The benefits of QFR guidance are supported in a recent study that showed that a QFR-guided strategy of lesion selection for PCI improved two-year clinical outcomes, including reduction in myocardial infraction and ischemia-driven revascularization, when compared with standard angiography guidance alone.2 Accessed May 2024.
To our knowledge, no studies have directly compared the right and left TRA for carotid artery stenting (CAS). We analyzed patient characteristics, clinical outcomes, and the presence of lesions on postprocedural diffusion-weighted imaging (DWI lesions).Results:A Patients who underwent proximal balloon-protected CAS were excluded.
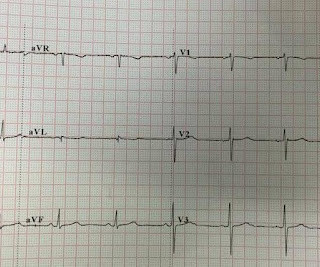
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. Normal FFR is 1.0 and an FFR below 0.75 in the study.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Outcome of case 2? Cath days later showed complete occlusion of the LAD, stented. Normal vitals. This one, too, is a swirl pattern and diagnostic of LAD occlusion.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He was intubated in the field and sedated upon arrival at the hospital. Two subsequent troponins were down trending.
IntroductionThe optimal endovascular approach for wide‐neck intracranial aneurysms (IAs) during the acute phase of bleeding remains uncertain, and the use of stent‐assisted coiling or flow diversion is controversial due to antiplatelet therapy requirements and potential risks (1, 2). Of the patients, 60.5%
BACKGROUNDThe optimal endovascular approach for acutely ruptured wide‐neck intracranial aneurysms remains uncertain, and the use of stent‐assisted coiling or flow diversion is controversial due to antiplatelet therapy requirements and potential risks. Stroke: Vascular and Interventional Neurology, Ahead of Print. Of the patients, 60.5%
Total endovascular reconstruction (TER) is increasingly feasible but mid-term and long-term outcomes have not been reported.Methods:Data from all patients treated with carotid CTO treated with TER over the past 18years were collected in a database.
ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. The patient was referred immediately for cath which revealed RCA occlusion that was stented. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1.
Due to the rarity of iatrogenic CeAD, existing literature on management and outcomes is limited. Of the 32 patients, 9(28.1%) had dissection with diagnostic angiograms, 6(18.8%) endovascular thrombectomy, 15(46.9%) aneurysm treatment, and 2(6.3%) angioplasty with or without stenting. Only 4(12.5%) were treated with hyperacute stenting.
Outcome In the EVAR group, 47 patients (95.92%) were successfully implanted with overlapping stents, and 2 patients died in the perioperative period. In addition, we summarized and analyzed their Computed Tomographic Angiography (CTA) results and perioperative complications.
Answer : There is very abnormal T-wave inversion in aVL which is typical of subtle transmural/subepicardial (due to occlusion) ischemia to the inferior wall. Similarly, the precordial T-wave inversions in V2-V4 are reciprocal to posterior wall transmural/subepicardial (due to occlusion) ischemia. An 80% thrombotic RCA was stented.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Lessons: 1. Lessons: 1.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. Cardiology: delayed cath = Non-STEMI Heres the interventional cardiology note describing the ECGs, management and outcome: He has had transitory peak T-waves, ST-segment elevation, and biphasic T-waves during recurrences of pain.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. It was opened and stented. This ECG is diagnostic of ischemia.
In his four months follow up clinic visit he had no further concerns of recurrent strokes or new symptoms.ResultsCarotid stump syndrome is a rare cause of cerebral and retinal ischemia; however, it must be considered in patients with recurrent ischemic strokes and chronic ipsilateral ICA occlusion.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." It was stented. Comment: most T-wave inversion is nonspecific, but not these ones! Gottlieb SO, et al.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. Peak troponin was 12 ng/mL. Stuckey, T., Zimetbaum, P. Tcheng, J.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Abstract 556.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. The so-called "ST Elevation" is really the end of the QRS of Right Bundle Branch block. --Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was This is a very common misread. New RBBB + LAFB is a very bad sign.
The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. 2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. But it is still STEMI negative.
An open 90% LAD was stented. A 51 year old male with h/o stent presented with 30 minutes of chest pain: Obvious anterolateral very acute STEMI with hyperacute T-waves He went for immediate PCI, with successful reperfusion of a 100% occluded proximal LAD, and a door to balloon time of 35 minutes. The LAD has reperfused early.
Leveraging Technology to Improve CABG Outcomes Viviany Taqueti, MD, MPH (Boston, MA, USA) 9:20 a.m. Women and CABG: A Comparison of Graft Conduit Outcomes from the National Adult Cardiac Surgery Audit Database Arnaldo Dimagli, MD (New York, NY, USA) 11:50 a.m. Panel Discussion 8:56 a.m. Panel Discussion 9:55 a.m. – 9:50 a.m.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. The lesion was stented. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated.
It was treated with and dual "kissing balloons" and drug eluting stents. Here is the post stent ECG: There is greater than 50% resolution of ST elevation (all but diagnostic of successful reperfusion) and Terminal T-wave inversion (also highly suggestive of successful reperfusion). TIMI flow is 0. Door to balloon time was 51 minutes.
Soviet biologist Trofim Lysenko famously rejected the objective reality of Mendelian genetics because it clashed with the Marxist philosophy that the environment, not genetics, was the primary determinant of outcomes. But what should matter is outcomes not diagnoses. Subscribe for free to receive new posts and support my work.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content