This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Myocardial ischemia may induce myocardial fibrosis, a condition that progressively leads to ventricular remodeling, heightening the risk of heart failure. The timely detection of myocardial fibrosis is crucial for intervention and improved outcomes. The results demonstrated tracer-specific uptake (SUVmax = 4.6)
What was the outcome?" Comparison Summary: ANTEROLATERAL ST CHANGES ARE NOW MORE PRONOUNCED, RATE DEPENDENT VS ISCHEMIC CHANGES Here is the Queen's diagnosis: The cath lab was activated: Culprit Lesion (s): Thrombotic 99% mid LAD stenosis with TIMI II flow Peak troponin not measured, unfortunately. I responded: "That is a tough one.
Coronary angiography gives a visual impression about the severity of the stenosis. But it need not imply the actual functional significance of the stenosis in terms of flow physiology. indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. Normal FFR is 1.0 and an FFR below 0.75
We performed this analysis to identify the prevalence of atrial fibrillation and associated outcomes in symptomatic internal carotid artery stenosis patients undergoing CAS or CEA.Methods:We analyzed the data from the National inpatient sample (NIS) between January 2016 to December 2021. versus 8.7%, p=0.41) and discharge home (32.4%
However, clinical outcomes remain similar. This study compares post-thrombectomy outcomes in both groups, matched by initial NIHSS scores.Method:From October 2017 to March 2023, we studied LVO cases undergoing thrombectomy for acute ischemic stroke. Successful recanalization was defined as Thrombolysis in Cerebral Ischemia score ≥2b.
This suggests further severe ischemia. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram.
Background:Inflammation, a key player in both acute and chronic cerebral ischemia, is activated in brain tissues by bilateral carotid stenosis (BCAS)- induced chronic cerebral hypoperfusion. Stroke, Volume 56, Issue Suppl_1 , Page ATP349-ATP349, February 1, 2025.
His response: “subendocardial ischemia. History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. Anything more on history?
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Wellen's syndrome is a Reperfusion syndrome.
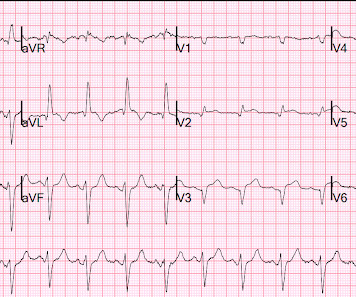
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This ECG is diagnostic of ischemia. LM: No significant stenosis.
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center. 24 and find out what it all means for your patients.
Likelihood of truth : High The flamboyant genius of Andreas Roland Gruntzig, from Zurich gifted us the path-breaking treatment modality for coronary stenosis five decades ago. Surprised and rejoiced to read this defiant article against ORBITA-2 from Impactful journal Circulation Cardiovascular Quality Outcomes. Come September 2024.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. ConclusionPTAS appears to be an effective and safe treatment for ICAD after MT in the posterior circulation both improving likelihood of good outcomes and overall survival.
The culprit lesion was a complex calcified mid LAD stenosis involving the first and second diagonal branches. Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Long term outcome unknown but obviously bleak. There was significant thrombus noted.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. The red arrow points to a 90% stenosis in the proximal segment of the LAD. The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”. RAO Caudal view: This is the RAO Caudal view.
There is normal R-wave progression in the precordial leads with no evidence of ischemia. COPD, Idiopathic PAH, acute or chronic PE, pulmonary valve stenosis, etc) 3) Conditions affecting RV myocardial contractility, such as ARVD or RV infarction The ECGs does not really show any signs of chronic RV dilation or hypertrophy.
T-wave inversion in V2 is inconsistent with early repol, and is typical of posterior ischemia. In addition, there is ST depression, diagnostic of ischemia, in V3-V6. It showed a 99% stenosis in the RCA, and proximal to a posterolateral branch. mm of ST elevation in inferior leads. There should be no doubt that this is OMI.
1-4 Surprisingly, serial angiographic studies have revealed that the plaque at the site of the culprit lesion of a future acute myocardial infarction often does not cause stenosis that, as seen on the antecedent angiogram, is sufficiently severe to limit flow. There may be a chronic tight stenosis and a non-obstructed lesion that thrombosed.
Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was Was the ST elevation due to transient demand ischemia, or is it false positive? It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. Does he need a stress test? --Is
Soviet biologist Trofim Lysenko famously rejected the objective reality of Mendelian genetics because it clashed with the Marxist philosophy that the environment, not genetics, was the primary determinant of outcomes. Marked differences can be seen in the prevalence of coronary artery stenosis at autopsy by age and gender.
This is ischemia until proven otherwise. Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. I learned that the patient is on Sotalol for control of PVCs. This explains the long QT.
Angiogram showed a critical LAD thrombotic stenosis. The patient went to cath and had a distal LAD 99% stenosis with thrombus and TIMI-2 flow. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing. He underwent CABG.
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). 90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX.
So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. EKG shown here: LAFB with no clear signs of OMI or ischemia. Queen of Hearts Interpretation: Would 20 minutes earlier diagnosis have made a difference in his clinical outcome?
Full case details and outcomes are below. Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia." Ongoing ischemia despite medical management has always been an indication for emergent cath, which is frequently ignored as it was in this case. Case 1: Case 2: Case 1: What do you think?
If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. Angiographic and clinical outcomes among patients with acute coronary syndromes presenting with isolated anterior ST-segment depressions. mm for women, 2.0 Pride et al.
We evaluated the primary outcome (cardiovascular death, myocardial infarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned men, and no ≥50% stenosis in 12.3% of invasive‐assigned women and 74.8%
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Evidence of acute ischemia (may be subtle) vii. These premonitory symptoms were negative predictors of adverse outcomes in EGSYS. Left BBB vi.
The patient was started on heparin for possible NSTEMI vs demand ischemia. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. What "initiates" the aortic stenosis cascade? increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.)
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content