This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
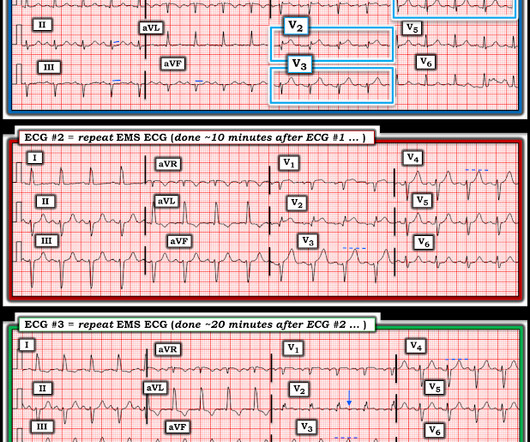
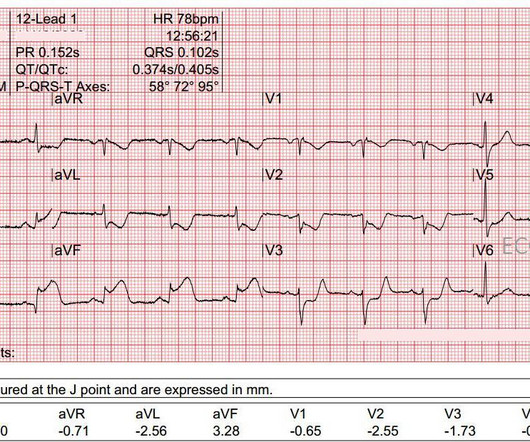
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. The patient survived with unknown long term outcome.
Cath lab declined as it is not a STEMI." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! It is a mass delusion.
The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch. Do you need posterior leads?
This study shows that for a transient STEMI ("complete normalization of ST segments"), it is not unequivocally necessary to activate the cath lab emergently. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded. See more cases of Transient STEMI here: [link]
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
There may be ischemia present, but it is not evident on the ECG. LVH and the diagnosis of STEMI - how should we apply the current guidelines? This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. How about diagnosing anterior STEMI in the setting of LVH? Birnbaum Y and Mahboob A.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. And as we have shown before, morphine leads to slower times to treatment and worse outcomes. 414 patients were included in the analysis.
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. There is about 1 mm of STE in aVR I con sidered but rejected subendocardial ischemia. Is it subendocardial ischemia, or inferior MI? Outcome : Was it RCA or LCX with inferior MI?
See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. Both support acute anterior STEMI. After the hyperacute phase, the ST segments rise and only fall with either 1) reperfusion or 2) prolonged ischemia leading to irreversible infarction.
Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
This was a machine read STEMI positive OMI. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. the investigators reviewed outcomes in 118 patients presenting with NSTEMI. His ECG is shown below.
1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
ST depression in the setting of acute transmural ischemia (STEMI) is almost ALWAYS due to reciprocal change. Outcome: The patient went to the cath lab, but we have no further followup. The elevation is higher in Lead III than in Lead II, a reliable sign of RCA occlusion. Reciprocal depression in Leads aVL and I.
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. The LAD has reperfused early. This was recorded 2.5
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? The patient stabilized and had a good outcome. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Long term outcome unknown but obviously bleak.
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. If I saw this without the STD V2-V4, I would not make anything of it, and even with that precordial STD, I am not convinced that it is a manifestation of ischemia. Because we are hypnotized the STEMI paradigm. "If
V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. However, the pattern is also seen in inferior OMI with right ventricular OMI. (V1
We have also shown several cases in which atrial flutter hides true, active ischemia. Is this inferor STEMI? Atrial Flutter with Inferior STEMI? The EM provider asked if the cardiologist thought it was a "STEMI." Long-term outcome is unknown. Christmas Eve Special Gift!! Tachycardia and ST Elevation.
This suggests further severe ischemia. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. Alternatively, it is a variant of diffuse subendocardial ischemia, with STE in V1 reciprocal to ST depression in inferior and lateral leads.
This ECG is diagnostic of diffuse subendocardial ischemia. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. We studied this and published the abstract below in 2010. Kurkciyan et al.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Opioids associate with worse outcomes in myocardial infarction , probably because they eliminate the pain signal that informs the clinician of the urgency of revascularization. Is there STEMI? Do not treat AIVR. Moffat, M.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Repeat ECG showing no STEMI, only non-specific ST-segment and T-wave abnormalities, unchanged from prior" Transferred to surgery for exploration but diagnostic studies were too indeterminate to be certain of intra-abdominal pathology. Trop T now very high, well into the range one sees with a STEMI; very unusual in type II MI.
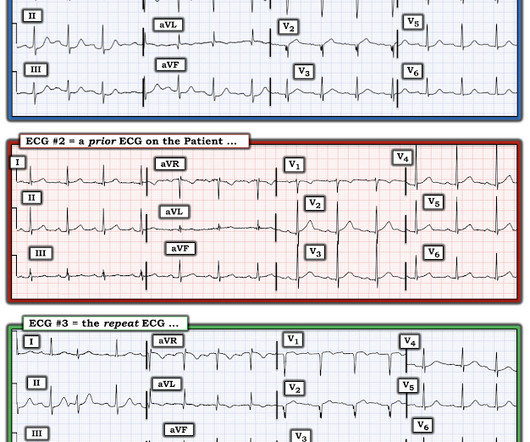
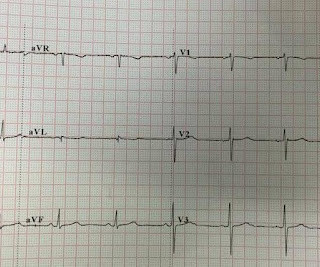
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." New ST elevation diagnostic of STEMI [equation value = 25.3 Computerized QTc = 417. Gottlieb SO, et al.
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. Anterolateral STEMI. He underwent PCI and had a good outcome. Ischemia comes and goes. mm of STE at 60 ms after the J-point in lead V3, 400 ms QTc, and 6 mm of R-wave amplitude in V4.
Just as hyperacute T-waves can be reciprocal to T-wave inversion ( last case ),T-wave inversion can be reciprocal to STEMI of opposite wall! Answer : There is very abnormal T-wave inversion in aVL which is typical of subtle transmural/subepicardial (due to occlusion) ischemia to the inferior wall. This case was sent by Arthur Lee.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Type B waves are deeper and symmetric.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. Therefore it is not a STEMI. Some are STEMI-equivalents.
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. This is a case I had quite a while back. There is a normal amount of ST elevation in the precordial leads.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
Outcome of case 2? Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! In addition — there is transmural ischemia of the septum , most often resulting from occlusion proximal to the 1st septal perforator branch of the LAD. Admitted for NSTEMI. Cath days later showed complete occlusion of the LAD, stented.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content