This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. He had been awakened by cough at 3 AM 2 days earlier.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiac arrest. Anterolateral STEMI. Ischemia comes and goes. He was defibrillated.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic @DidlakeDW A 50 y/o Male was taking his dog for a leisurely stroll through the park when he suddenly experienced new onset chest discomfort. it has been subsequently deemed a STEMI-equivalent.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. There is LBBB-like morphology with persistent patterns of subendocardial ischemia.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review by Dr. Stephen Smith @smithECGblog I was reviewing ECG’s in our LifeNet database and happened upon this one without any knowledge of clinical circumstances. 1] Here is the admitting ED ECG after cancellation of Code STEMI. ST-elevation, etc.)
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGBlog An adult female called 911 for chest discomfort and difficulty breathing. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. Wolters-Kluwer: Philadelphia, PA. [2]
One of my most talented readers is a health care assistant (a nursing assistant) who has taken a keen interest in ECGs. Trop T now very high, well into the range one sees with a STEMI; very unusual in type II MI. And they teach me a lot. He can beat nearly anyone. So you don't have to be highly trained. You don't have to be a genius.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered.
It had started just after nursing her newborn, about an hour prior, and she described it as a severe non-pleuritic “pressure” radiating to the back. This strongly suggests reperfusing RCA ischemia. A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. 24 yo woman with chest pain: Is this STEMI? This is not "diffuse", this is simply anterior, lateral, and likely apical.
Our triage nurse therefore ordered an ECG for him (which is standard in our dept for epigastric pain patients): What do you think? The STEMI criteria in normal conduction are only 75% sensitive for OMI!! They cannot be assumed due to LV strain ( and they cannot be assumed to represent ischemia ).
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
The nurse alerted the MD because the patient was still symptomatic, diaphoretic and “looking unwell”. This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram. Discharge diagnosis was ‘STEMI’, even though no ECG ever met STEMI criteria. What do you think? Shroff, G.
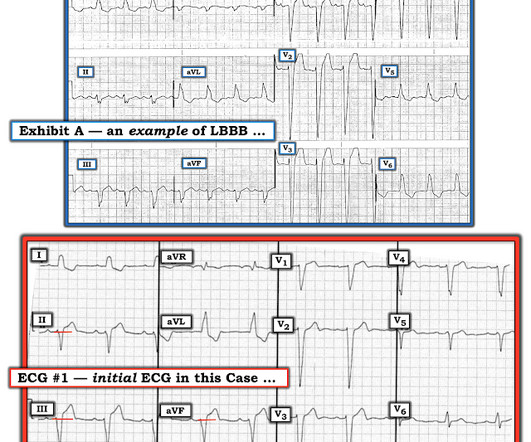
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria. There is evidence of transmural ischemia of the posterior wall as well. Lucky Hans.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content