This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque.
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Diagnosis and treatment of ischemia-producing coronary stenoses improves 5-year survival of patients undergoing major vascular surgery.” 101272, [link].
This EKG is diagnostic of transmural ischemia of the inferior wall. The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Lead I also shows reciprocal ST depression.
Angiography has limitations that make it difficult to determine the true artery size and the makeup of the plaque, and is suboptimal in determining whether the stent is fully expanded post-PCI and identifying other complications that affect the safety and effectiveness of the procedure.
This suggests further severe ischemia. MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. And yet the arteries remain open.
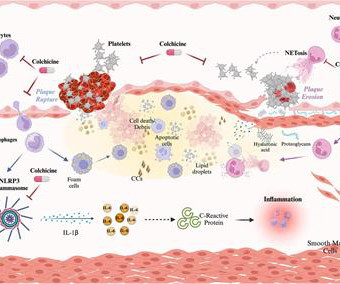
ACS may arise from the disruption of an atherosclerotic plaque, ultimately leading to acute ischemia and myocardialinfarction. Colchicine exerts anti-inflammatory properties affecting both the myocardium and atherosclerotic plaque by modulating the activity of monocyte/macrophages, neutrophils, and platelets.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
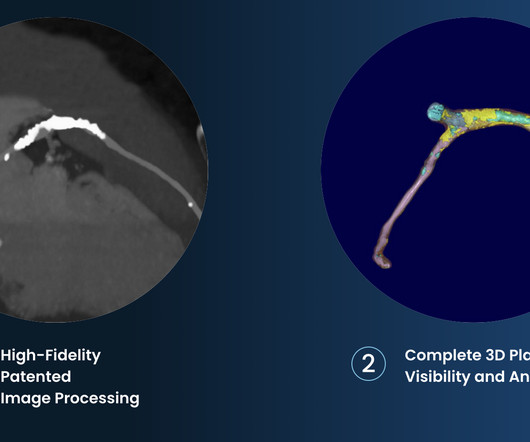
tim.hodson Tue, 10/01/2024 - 10:50 PHOTO CAPTION: The Elucid PlaqueIQ user interface is a fully interactive visualization of the patient’s coronary anatomy, showing specific plaque type and amount across various views to inform physician assessment of risk and patient-specific treatment pathway.
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. Eur J Emerg Med.
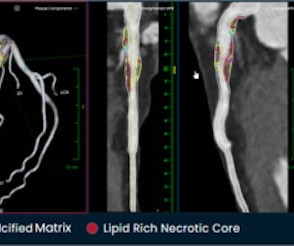
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. There are 3 types of coronary atherosclerosis visible on CTCA: Calcified Plaque - Easily Identified on both CT CAC & CTCA scans. Subscribe now How Often Does A CT CAC Scan Miss Plaque?
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4
Without oxygen, the cells would quickly die, leading to a heart attack (myocardialinfarction). For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). It can only be seen by IVUS. MINOCA has many etiologies. Learning Points: 1.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). The primary care physician's note indicates low suspicion for cardiac ischemia, but "for completion, check troponin and ECG." If an ECG was obtained in the office, it was not saved.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. As there was ruptured plaque, this is NOT Prinzmetal's angina.
This is diagnostic of myocardialinfarction. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point.
Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. See P.S. below ) == P.S. : I believe I found another example of ischemia-induced J waves ( See Oct.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Comparison of the QRS complex, ST-segment, and T-wave among patients with left bundle branch block with and without acute myocardialinfarction.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found.
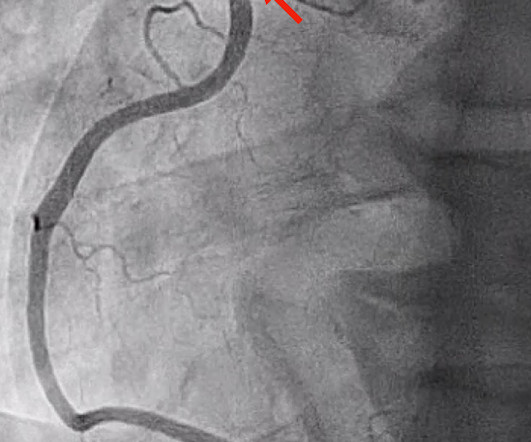
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI. He was successfully stented.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. SanzRuiz, R., Solis, J., &
Influenza-like illness can also trigger plaque rupture. Prevalence and outcome of patients with non-ST segment elevation myocardialinfarction with occluded culprit artery - a systemic review and meta-analysis. This means that, in the United States alone, of 500,000 NSTEMI, 170,000 do not get the care they deserve.
But it also shows a massive area of total ischemia in the LAD territory: CT shows the infarct The CT is with contrast, which increases density (which looks more white). This was ruptured plaque with thrombus. Most dissections which cause coronary ischemia are into the RCA ostium ("ostium" = locations of takeoff of the vessel).
Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved. This was attributed to a "Type 2 MI", which is acute MI that is not due to ruptured plaque, but rather due to "supply demand oxygen mismatch". Next day, with K = 4.6
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content