This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
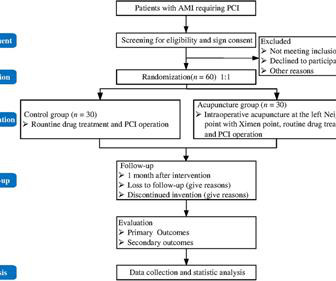
BackgroundSlow flow/no-reflow (SF-NR) during percutaneous coronary intervention (PCI) is associated with poor prognosis of patients with acute myocardialinfarction (AMI). Incidence of SF-NR is the primary outcome for this study. Currently, effective treatment is not available for SF-NR.
What was the outcome?" There is akinesis of the distal septum, anterior, apex, and distal inferior wall consistent with LAD territory ischemia or infarction. How large is the infarct? This was sent to me without any info while I was out and about, and I looked at it on my phone. I responded: "That is a tough one.
Myocardialischemia may induce myocardial fibrosis, a condition that progressively leads to ventricular remodeling, heightening the risk of heart failure. The timely detection of myocardial fibrosis is crucial for intervention and improved outcomes. The results demonstrated tracer-specific uptake (SUVmax = 4.6)
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. If I saw this without the STD V2-V4, I would not make anything of it, and even with that precordial STD, I am not convinced that it is a manifestation of ischemia. This is a HUGE myocardialinfarction.
There may be ischemia present, but it is not evident on the ECG. In this paper, Dr. Birnbaum writes: "In patients with ACS without LVH, ST depression with negative T waves in the lateral leads is a sign of sub-endocardial ischemia and is an independent predictor of adverse outcome [11 – 13]. Notice the S-wave in V2 is 45 mm.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center. 24 and find out what it all means for your patients.
The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Wellen's syndrome is a Reperfusion syndrome.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. The ECG is diagnostic of occlusion myocardialinfarction (OMI).
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. Eur J Emerg Med.
BACKGROUND:Cardiolipin is a mitochondrial-specific phospholipid that maintains integrity of the electron transport chain (ETC) and plays a central role in myocardialischemia/reperfusion injury. Tafazzin is an enzyme that is required for cardiolipin maturation.
There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). Opiates are associated with worse outcomes in MyocardialInfarction. It is one of the few OMI patterns that is really well described: de Winter’s T-waves.
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardialinfarction, probably old." Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Long term outcome unknown but obviously bleak.
This suggests further severe ischemia. associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Downstream vasospasm?
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). Guagliumi, G., Iwaoka, R. O’Neill, W.
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
hours later, after PCI: There is a significant QS-wave in V2, with some persistent ST elevation, suggesting incomplete small vessel reperfusion and significant infarction. The patient continued to have ischemia after PCI, and in fact had an episode of polymorphic VT shortly after while in the ICU. This was recorded 2.5
But ECGs interpretation is often conflated with clinical assessment, so if patients don’t present with chest pain the ischemic changes are not seen or are attributed to something other than ischemia. Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States. Circulation 2007 2.
Risk ratios (RRs) and mean differences with 95% CIs were computed for binary and continuous outcomes, respectively.RESULTS:Five randomized controlled trials with a total of 5727 patients were included, of whom 51.1% of patients had evidence of ischemia on a prior functional test. were referred to CCTA and 22.5% 0.98];P=0.043).
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. Outcome There are differing data about prognosis of CS in STEMI vs NSTEMI. Circ Cardiovasc Qual Outcomes.
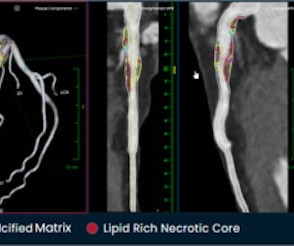
I believe plaque quantification has the potential to greatly improve outcomes for patients while providing tremendous savings to the healthcare system.” Armed with additional data on vulnerable plaque components, we can make more informed treatment decisions on drug therapy selection or the need to send the patient to the cath lab.
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Academic Emergency Medicine 27(S1): S220. Abstract 556.
This is diagnostic of myocardialinfarction. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). 1] The patient did not have a good outcome because their ECG was labeled ‘normal’ but in spite of it. JAHA 2022 Grosmaitre P et al.
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With MyocardialInfarction With Nonobstructive Coronary Artery Disease. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Outcome of our case Once the type 2 SCAD was identified, the heparin drip was stopped. Lobo et al.
These methods only alleviate symptoms of heart failure and myocardialischemia and improve patients' quality of life by partially restoring myocardial reperfusion. The main content of this paper is to explore the application of stem cells and gene technology in the treatment of myocardialinfarction (MI).
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. years, with 21.1% occurring within 30 days after PCI. years, with 6.3%
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion MyocardialInfarction (Versus Nonocclusive Ischemia). Ventricular fibrillation is a common outcome in OMI and should greatly heighten the suspicion for ischemic heart disease even in the absence of profound ST elevation. =
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing. Outcome : The third troponin I, drawn 4.5
This case was texted to me by one of our residency graduates, and with the outcome, so I don't know how I would have interpreted it blindly. Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. is worrisome!
Full case details and outcomes are below. Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia." Next trop 85,528 ng/L (consistent with a massive myocardialinfarction), none further measured. Case 1: Case 2: Case 1: What do you think? Smith's response was: "OMI Mimic."
If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. Diagnosis of acute myocardialinfarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads.
The largest trial to examine the impact of colchicine in acute myocardialinfarction (MI) found that both acute and long-term colchicine use did not reduce cardiovascular death, myocardialinfarction, stroke, or ischemia-driven revascularization.
I suspect its use will rapidly accelerate given study after study now showing reductions in death, stent thrombosis, and nearly every other adverse outcome after PCI when intravascular imaging is used. Currently,IVI is performed inonly 20 to 25 percent of these cases in the United States.
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
BackgroundAcute psychological stress may induce physiological changes predisposing individuals to adverse health outcomes through hemodynamic and vascular effects. The outcome was a composite of cardiovascular death, nonfatal myocardialinfarction, and heart failure hospitalizations during followup.
The 2 coprimary outcomes were target lesion revascularization and myocardialinfarction. The secondary outcomes included ischemia-driven target lesion revascularization, target vessel myocardialinfarction, death, cardiac death, target vessel revascularization, stent thrombosis, and major adverse cardiac events.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Accessed May 2024. Kirtane, Yongjian Wu, William Wijns, Weixian Yang, Martin B. Leon, Shubin Qiao, Gregg W.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content