This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
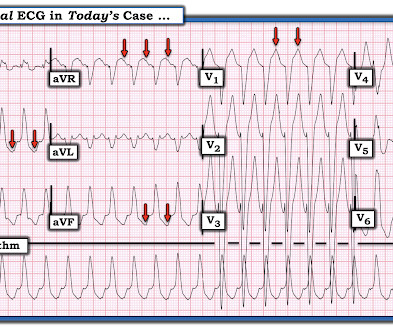
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation.
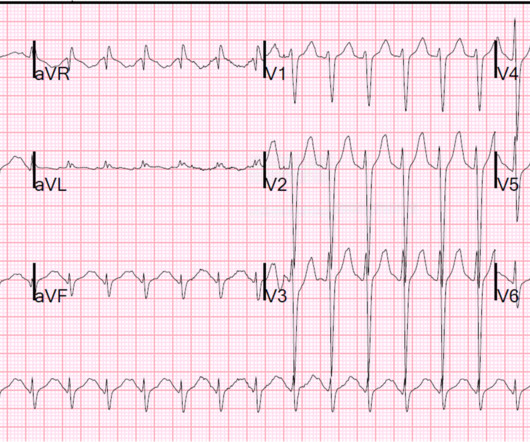
CASE CONTINUED She was admitted to the ICU. Even with tachycardia and a paced QRS duration of ~0.16 Smith has provided excellent overview of measuring and correcting QT interval in scenarios where QRS duration is prolonged (e.g., LBBB, ventricular pacing, etc.)." J Am Coll Cardiol.
A young male with unknown past medical history presents with AMS and tachycardia. There is sinus tachycardia, a prolonged QRS (computer read it as 114 ms, previous ECG with 102 ms). But because the physicians were so focused on his tachycardia, meth use, and rhythm, they did not look for or appreciate the findings of TCA overdose.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval.
The patient was upgraded to the ICU for closer monitoring. and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE. Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP. inverted T-waves in V1 and V2, 1.8;
There is a regular, wide complex, (mostly) monomorphic tachycardia. The differential of wide, regular, monomorphic tachycardia is: VT or SVT with aberrancy, all +/- hyperkalemia (see diagrams below). He made it to the ICU, however the patient unfortunately expired approximately 24 hours after ICU admission.
A 65 y/o Female was admitted to the ICU for septic shock. From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. Question 2: What explains the conduction abnormalities?
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course.
Interpretation: There is sinus tachycardia, with right bundle branch block (RBBB). Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. She was pulseless, with a narrow complex tachycardia on the monitor. She was intubated.
The findings include sinus tachycardia, characteristic QRS morphology most diagnostic in V3 with a small R wave followed by a very large S wave with a convex upward ST segment morphology, ST segment strain morphology in the inferior and anterior leads leading to deep symmetric T-wave inversion. and tachycardia, 1.8. incomplete RBBB 1.7
Prior ECG on file: Sinus tachycardia, imperfect baseline, otherwise unremarkable. Sinus tachycardia with unequivocal evidence of hyperkalemia, including widened QRS with "pulled apart" morphology (widened QRS) compared to baseline, as well as clearly peaked T-waves. He required a low dose norepinephrine drip to maintain BP.
2] But there is also Sinus Tachycardia! Thankfully, the patient experienced an uncomplicated ICU stay and subsequently made a full recovery. This makes occlusive MI (in isolation) less likely and merits further investigation, as well as intensified ECG scrutiny – specifically, the T waves. The serum K returned 8.7,
(Ken Grauer points out that this 5th beat appears to be due to an early atrial beat and that these early beats continue for a few beats, suggesting a short run of atrial tachycardia.) and the 2021 YouTube Review by ICU Advantage on "Temporary Pacemakers: Modes and Basic Settings".
After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. A Very Wide Complex Tachycardia.
The patient was managed in the ICU and had serial troponins. In such cases, it is common for tachycardia to exaggerate the ST Elevation And, in fact, there was no new acute MI at this visit - troponins did not rise again. It is not yet available, but this is your way to get on the list. He had no more ECGs recorded. First was 2.9
in the ICU but survived with excellent function. That said — the heart rate is significantly faster than it was for the prior 2 tracings ( ECGs #1 and #3 ) — so there is really no way to distinguish what might represent ST-T wave changes due to tachycardia vs evolution of the patient’s underlying disorder.
A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid. One looks for sinus tachycardia and diffuse low voltage but many conditions produce these nonspecific findings.
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
2025.110515 [link] Abstract Objective: The administration of amiodarone or lidocaine is recommended during the resuscitation of out-of-hospital cardiac arrest (OHCA) patients presenting with defibrillation-refractory or recurrent ventricular fibrillation or ventricular tachycardia. DOI: 10.1016/j.resuscitation.2025.110515
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content