This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
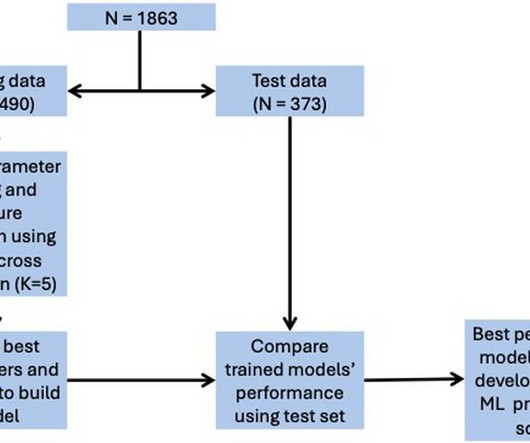
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for ICU admission, and 0.74 for in-hospital mortality, 0.78 for LVEF < 40%.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. The LAD has reperfused early. This was recorded 2.5
Subtle as a STEMI." (i.e., A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." The patient was upgraded to the ICU for closer monitoring. If this EKG were handed to you to screen from triage without any clinical information, what would you think?
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Is it STEMI? See these other relevant cases: What are these bizarre bigeminal PVCs?? Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest.
and ICU-related anxiety stand apart in this scientific comical game of ruling out a cardiac emergency. More than that, the adversities of the tense investigative protocol can convert a misdiagnosis into a real one because that sadly includes even an overzealous poking right at the mouth of the coronary artery just o exclude a non existing MI.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Thankfully, the patient experienced an uncomplicated ICU stay and subsequently made a full recovery. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest.
I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. Her repeat ECHO showed an improving EF of 37%.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. From Ken Grauer ( See below ) — with this Figure adapted from LITFL.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. The facility was not pressed to activate emergent transfer for PCI since the pain was improving and suggested we optimize pain control and admit to the Cardiac ICU. Lupu L, et al. mg/dL, K 3.5
The patient was managed in the ICU and had serial troponins. (THE PM CARDIO OMI AI APP) If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list. First was 2.9
in the ICU but survived with excellent function. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs.
Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab. His troponin I peaked at 97 ng/mL (very large MI!). His follow up ECHO the next day revealed an EF of 24% and a posterior wall motion abnormality.
A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid. Approximately 500 mL of serous fluid was withdrawn from the catheter with immediate normalization of all vital signs. mm STE depression in aVL.
and the patient was given more insulin/dextrose/calcium and admitted to ICU. Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! HyperKalemia with Cardiac Arrest. References 1. Lindner et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content