This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
They included randomised controlled trials that enrolled adults undergoing major cardiac surgeries and reported postpericardiotomy syndrome, pericardial effusion and pericarditis as primary or secondary outcomes. to 0.81) and may prevent postoperative pericarditis (RR 0.66, 95% CI 0.45 Pairs of reviewers screened eligible studies.
mm has been described in normal subjects) Overall impression: In my opinion and experience, this ECG most likely represents a normal baseline ECG, but with a small chance of pericarditis instead. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant."
She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. She had an uneventful ICU course and was extubated for ongoing care with the inpatient psychiatric service.
A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid. She was diagnosed with pericarditis and spent one day in the hospital without events. Much more classic findings of pericarditis. mm STE depression in aVL.
You do NOT see this in normal variant STE, nor in pericarditis. The patient was managed in the ICU and had serial troponins. Here is the computer interpretation: (Veritas algorithm) This is what I said: "This is diagnostic of an acute inferior MI. There is upsloping ST elevation in III, with reciprocal ST depression in aVL.
The patient was upgraded to the ICU for closer monitoring. Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis 31 Year Old Male with RUQ Pain and a History of Pericarditis. Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP. What is the Diagnosis?
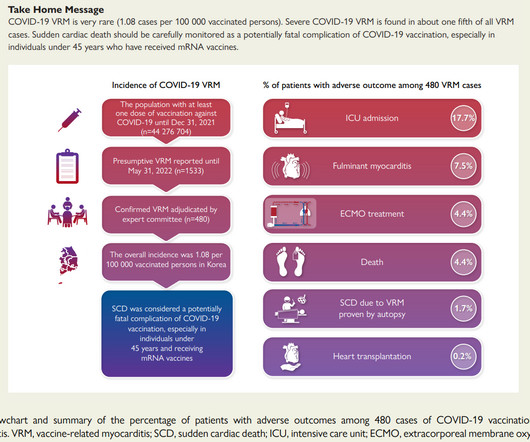
The KDCA also established a reporting system with a legal obligation for special adverse events including myocarditis and pericarditis after COVID-19 vaccination. Of the 1533 cases of potential vaccine myocarditis reported, the expert adjudication committee confirmed 480 Covid 19 VRM cases.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content