This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
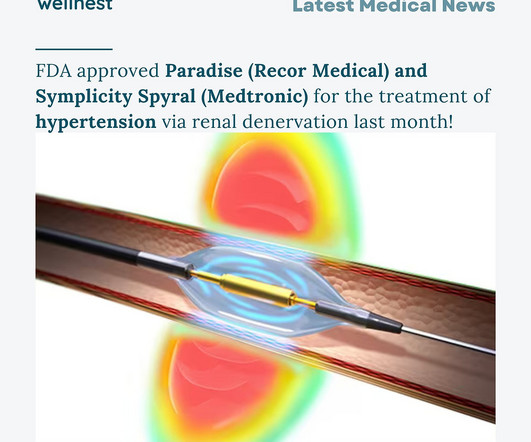
Centers for Medicare & Medicaid Services (CMS) have granted the company’s Paradise Ultrasound Renal Denervation system a Transitional Pass-through (TPT) payment. The approval of TPT offers incremental reimbursement payments for outpatient procedures performed with ultrasound renal denervation for Medicare fee-for-service beneficiaries.
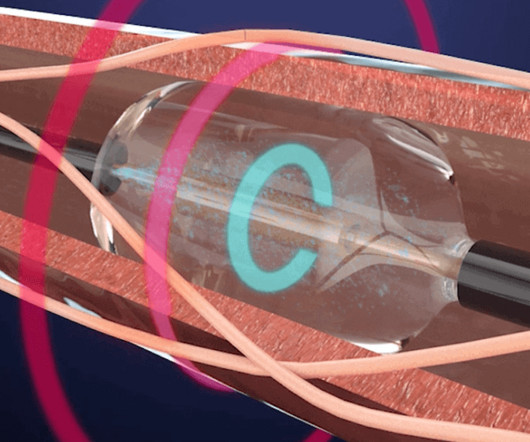
and the first on the West Coast to use a new device aimed at lowering blood pressure in patients with difficult-to-treat hypertension. At the tip of the catheter is an ultrasound transducer that is covered by a water-filled balloon to cool and help protect the lining of the renal artery. The entire procedure takes about an hour.
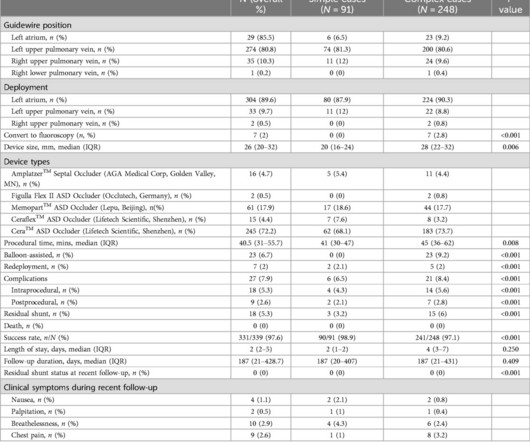
IntroductionZero-fluoroscopy, exclusively ultrasound-guided atrial septal defect (ASD) catheter closure has been reported. Complex cases included patients with large defects (25mm), multiple or fenestrated ASDs, deficient posterior-inferior rim <3mm, deficient retro-aortic rim <5mm, pulmonary hypertension, septal malalignment, and pregnancy.
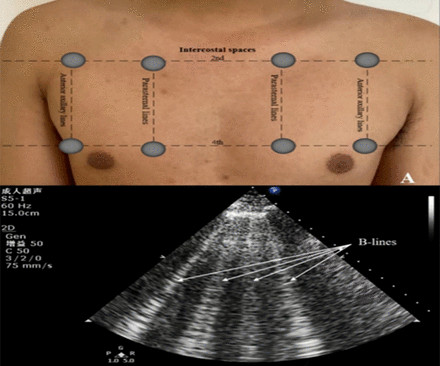
Objectives Prognostic impact of lung ultrasound-derived B-lines (LUS-BL) in heart failure with mildly reduced left ventricular ejection fraction (HFmrEF) patients remains elusive. Older age, hypertension (HR=2.06, 95% CI 1.31 We evaluated the correlation between LUS-BL and prognosis in HFmrEF patients.
Renal denervation (RDN) is an adjunct treatment for hypertension (HTN) that involves catheter ablation of the sympathetic plexus in the adventitia of the renal arteries using radiofrequency (RF) or ultrasound waves.
We report a case of TRAD in the early postoperative period, which was successfully managed with intravascular ultrasound-assisted endovascular intervention.Case presentationA 38-year-old man underwent HLA-compatible living kidney transplantation. Most cases are managed by operative repair.
These groundbreaking developments offer a paradigm shift in the management of resistant hypertension, especially when it is extremely difficult to achieve blood pressure control through conventional means, such as lifestyle modifications and various drug therapies. But what is resistant hypertension, and why does it require renal denervation?
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound. So hypoxia without B lines on lung ultrasound strongly weights toward PE.
A new screening algorithm for preeclampsia combining maternal history, ultrasound data and several tests for blood markers may better predict the majority of preeclampsia cases in the first trimester of pregnancy, when it may still be preventable, according to new research published in Hypertension.
He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. Furthermore, the patient has no chest pain (certainly many STEMI do not have chest pain, but it should always make you especially scrutinize the ECG and the clinical situation) and there was severe hypertension.
Background:In Central Asia, hypertension accounts for 14.5% Second group (n=24) consisted of pregnant women with chronic hypertension/CHT. Endothelial function was analyzed using a flow-mediated dilation (FMD) test by using ultrasound system Simens Acuson X700 and the level of nitric oxide (NO) concentration.
Background:The RADIANCE-HTN SOLO, RADIANCE-HTN TRIO, and RADIANCE II randomized, sham-controlled trials independently met their primary endpoint of a greater reduction in daytime ambulatory systolic blood pressure (SBP) at 2 months after ultrasound renal denervation (uRDN) in patients with hypertension.
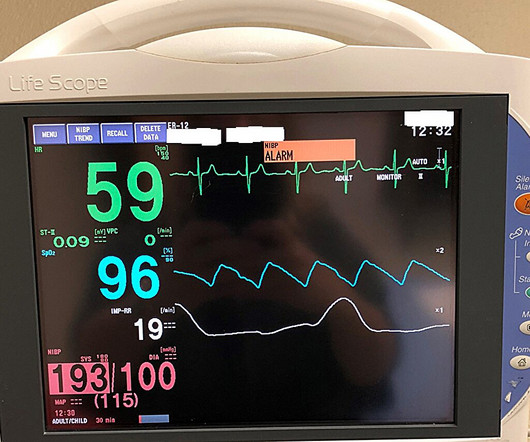
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A 56 year old male with PMHx significant for hypertension had chest pain for several hours, then presented to the ED in the middle of the night. A bedside cardiac ultrasound performed by a true EM expert (Robert Reardon, who wrote the cardiac ultrasound chapter in Ma and Mateer) showed an inferior wall motion abnormality.
Renal denervation (RDN) is intended for hypertension that can’t be controlled by conventional therapies, either due to ineffectiveness, side effects, or adherence issues RDN lowers blood pressure by denervating the sympathetic nerves surrounding renal arteries, reducing overactivity that can lead to hypertension Recor’s ultrasound-based Paradise System (..)
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema.
Right ventricular myocardial work (RVMW) assessed by transthoracic echocardiography allows to study the right ventricular (RV) function using RV pressure-strain loops. The assessment of these novel indexes of.
A 30-something woman with chest pain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chest pain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism.
ET Main Tent (Hall B1) Effect of Gamification, Financial Incentives or Both Combined to Increase Physical Activity Among Patients with Elevated Risk For Major Adverse Cardiovascular Events.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chest pain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain.
Patients with dextrocardia present a diagnostic challenge, particularly in the context of acute coronary syndrome.Case Presentation:A 49-year-old male with a medical history of dextrocardia, hypothyroidism, dyslipidemia and hypertension was referred to a cardiologist by his primary physician due to a 3-week history of unstable angina.
This was sent by a recent ultrasound fellow, asking for my ECG diagnosis. He stated that it is "an acute change from previous" in an elderly smoker with hypertension, syncope, and abdominal pain. First, there is some lead placement problem with V2, but I'm not sure exactly where it belongs!
My opinion was that it was not a cath lab case, but I did suggest they do a bedside ultrasound to look for an anterior wall motion abnormality. I had not seen the cardiac ultrasounds at this time. I did not have more information at the time. To the ED providers, the patient denied CP, SOB, or drug use.
Stavros Zanos is the senior author on the new bioelectronic medicine ultrasound paper. Credit: Feinstein Institutes) milla1cf Wed, 05/08/2024 - 10:57 May 8, 2024 — Ultrasound could one day complement or even replace drugs to treat diseases.
Tricuspid regurgitation jet velocity and pulmonary regurgitation end diastolic velocity indicating pulmonary hypertension are also taken as surrogates of left atrial pressure in the absence of pulmonary disease. J Cardiovasc Ultrasound. J Cardiovasc Ultrasound. Ha J et al. 2009 Sep;17(3):86-95. Park JH et al. Møller JE et al.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chest pain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. Here are a few clips.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
This suggests that there is pulmonary hypertension and thus possibly RVH. So we did a bedside cardiac ultrasound. In a patient with RVH — the finding of a qR pattern has been closely correlated with pulmonary hypertension. As per Dr. Smith — Chart review and repeat formal Echo confirmed marked RVH with pulmonary hypertension.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. On medic arrival, she walked out of the house in no distress, but was diaphoretic.
Case submitted and written by Dr. Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Smith comment: This patient did not have a bedside ultrasound. In fact, bedside ultrasound might even find severe aortic stenosis. What should be done?
I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram. Past medical history included diabetes and hypertension. As for the ECG, it could represent OMI, but RBBB is also a clue that it may be PE.
Cupid EHR from Epic boasts the following: Cloud-based EHR Offers integrated order entry, scheduling, procedure documentation, structured reporting, and data analytics for cardiology practices Supports a wide range of workflows, including Echocardiograms, Ultrasound vascular, Cardiac Cath, stress testing, Electrophysiology, and structured documentation (..)
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
ALL TROPS WERE UNDETECTABLE A formal ultrasound was done: Normal estimated left ventricular ejection fraction at rest. The complete lack of chest pain in the history in this patient who has longstanding hypertension strongly suggests that rather than ischemia, this symmetric T wave inversion reflects LV “strain” from marked LVH.
BackgroundArterial hypertension is characterized by microvasculature changes and reduced tissue perfusion. It is unknown whether a sexual dimorphism of renal microcirculation is present in patients with arterial hypertension. We measured the PI at rest and during a 2minute CPT in patients with arterial hypertension.
Abstract Aims Recent studies have shown that lung ultrasound-assessed pulmonary congestion is worse in heart failure when pulmonary vascular resistance (PVR) is increased, suggesting a paradoxical relationship between right heart failure and increased lung water content.
“We are witnessing a paradigm shift in how valvular heart diseases are diagnosed and treated,” said Partho Sengupta , Henry Rutgers Professor of Cardiology and chief of the Division of Cardiovascular Disease and Hypertension at Rutgers Robert Wood Johnson Medical School.
All subjects underwent a lipidomic analysis using ultra-high performance liquid chromatography–electrospray ionization tandem mass spectrometry, carotid ultrasound (mode B) to assess SCA, and clinical assessment.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. Chest Pain – Benign Early Repol or OMI?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content