This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
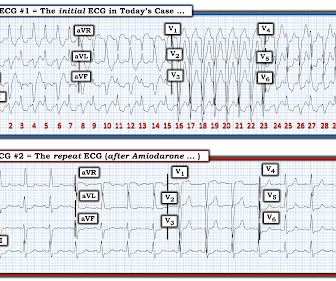
So, we can assume the patient was probably being treated for angina, heart failure, and hypertension. The ECG : The first impression is that is a regular WIDE COMPLEX TACHYCARDIA. It pays to take a moment to consider the possibility of REGULAR REALLY WIDE COMPLEX TACHYCARDIA (RRWCT) before making a treatment decision.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160. SVT with aberrancy?
A woman in her mid-60s with a history of paroxysmal atrial fibrillation and hypertension presents with 3 days of nausea, vomiting, and diarrhea. What would you do next?
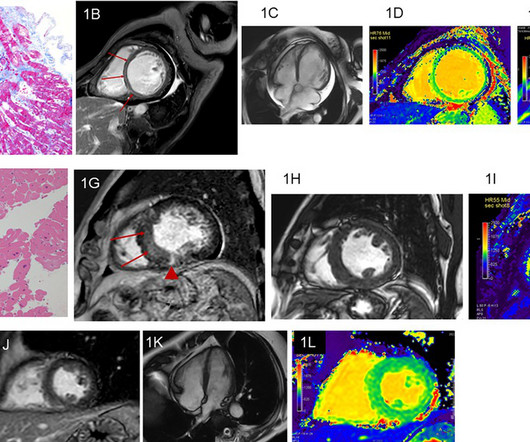
DCM had higher T1 and lower vGLNU than HC. When compared with TIC, DCM showed significantly higher LVEDV and LVEDVi. ROC analysis revealed that LVEDV and vGLNU provided high specificity for differentiating DCM from the other etiologies.ConclusionNative T1 mapping and its texture analysis may be valuable for differentiating between DCM and HC.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock).
Here is his ED ECG: There is sinus tachycardia. Furthermore, the patient has no chest pain (certainly many STEMI do not have chest pain, but it should always make you especially scrutinize the ECG and the clinical situation) and there was severe hypertension. The hypertension alone is the likely etiology of the pulmonary edema.
Multifocal Atrial Tachycardia 2. MAT almost always occurs in one of 2 common clinical scenarios : i ) Severe pulmonary disease ( ie, COPD, long-term asthma; pulmonary hypertension ) ; or , ii ) Acutely ill patients with multisystem disease ( ie, patients with sepsis; shock; electrolyte and/or acid-base disorders ).
She was noted to be in heart failure, with hypotension and tachycardia. Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension. With decompensated heart failure and adequate prior anticoagulation, the patient underwent direct current synchronised cardioversion for her arrhythmia.
NOTE: For more on ECG recognition of RVH and/or pulmonary hypertension ( re the qR pattern in lead V1 ) — See ECG Blog #234 and Blog #248. Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. This is precisely what we see in Figure-6. Unfortunately — I lack this information.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. However, underlying lesions such as hypertension, mitral valve disease, COPD, ASD, and TR greatly influence the degree of atrial enlargement. However, in cases of lone AF, AF in hypertension, or chronic AF, both atria tend to dilate equally.
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chest pain radiating to his back. The constellation of dyspnea, tachycardia, and (relatively) low voltage on ECG should prompt immediate evaluation for pericardial effusion and tamponade. He had associated nausea, vomiting, and dyspnea.
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? A VSR is more likely to occur in patients who are older, female, hypertensive, have chronic kidney disease, and have no prior history of smoking.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. What is the rhythm? Smith : Are they P-waves?
Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. Risk Reduction Data from wearables can identify potential risks, such as undiagnosed arrhythmias or hypertension, allowing healthcare teams to address these issues before surgery.
A 70-year-old male with a history of hypertension, hyperlipidemia, coronary artery disease, and CABG, presented with symptoms of moderate-intensity palpitations that terminated with Valsalva maneuvers. He was noted to have supraventricular tachycardia (SVT) on an event monitor.
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
He was counseled to abstain from cannabis use.Conclusion:At low to moderate doses, cannabis can lead to a surge in sympathetic activity causing tachycardia and hypertension, while parasympathetic activity is predominant at higher doses, causing bradycardia and hypotension.
Results Patients who developed >20% RV pacing ( n =148, 1.3%) had a higher likelihood of being older, male, and with a history of syncope, ventricular tachycardia or cardiac arrest, hypertension, previous or ongoing AF, and longer PR, QRS duration and BUN level ( p 230ms, history of AF, ongoing AF at time of implant, history of VT or cardiac arrest, (..)
Propensity score-matched analysis (PSM) (1:1) was performed with matching for age, gender, race, BMI, hypertension, diabetes mellitus, chronic kidney disease, hemoglobin level, low-density lipid (LDL) level, left ventricular ejection fraction, and various drugs including ACEi, ARBi, ARNI, beta-blockers, and diuretics. years, with 49.27% men.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”.
edits by Meyers A woman in her 60s with a history of chronic atrial fibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. Tachycardia and ST Elevation. Christmas Eve Special Gift!!
In the context of today's case — these P waves are diagnostic of RAE = P Pulmonale ( See ECG Blog #75 ) and almost certain associated pulmonary hypertension. Retrospectively — I interpret this 1:1 retrograde conduction as diagnostic of a reentry SVT rhythm as the etiology of the initial tachycardia.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia (or nearly) 2. Tachycardia, = 1.8. An ECG was texted to me (Smith) without any clinical information: What did I say?
Chronic RVH is due to chronic pulmonary hypertension, and these patients are extremely difficult to manage when they are acutely ill. Obviously he has multiple reasons to have pulmonary hypertension. But in pulmonary hypertension, RV perfusion is greatly diminished, especially when there is hypotension. How about management?
Crochetage sign on ECG in ASD ECG in ASD with severe pulmonary hypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen. Sharp P waves in V1 and 3 mm tall P waves in lead II suggest right atrial overload.
Past medical history included diabetes and hypertension. There is sinus tachycardia at ~100/minute. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenic shock ). Vitals were normal. The initial ECG for Patient #2 also shows RBBB.
His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. I suspected no OMI, that this could be due to LVH plus tachycardia. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use. On arrival to the ED, the patient was diaphoretic, tachycardic.
This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. Acute coronary occlusion (especially during reperfusion) is very rarely accompanied by tachycardia. and tachycardia, 1.8. The T-waves simply look different in Wellens'.
Right atrial hypertrophy as in tricuspid stenosis, pulmonary stenosis and pulmonary hypertension. But in a VSD with pulmonary hypertension A wave is not prominent. One is ventricular tachycardia with regular retrograde activation. We noted that prominent V waves or CV waves can occur in tricupsid regurgitation.
The cyanosis in Ebstein’s anomaly, is usually not due to pulmonary hypertension, but because tricuspid regurgitation jet is directed across the atrial septal defect. This is one important cause of supraventricular tachycardia in Ebstein’s anomaly. Electrophysiological study will show that, and this pathway can be ablated.
Vital signs were noted to be unremarkable with respect to any hypo-hypertensive crisis, hypoxia, etc. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Fire/EMS crews found him clammy and uncomfortable.
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. This results in Type I MI.
This ECG has Q-waves, but they are not very wide nor very deep, and so I doubt that the inferior STE is due to old MI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chest pain and shortness of breath off and on over the past three days, with associated vomiting. The rhythm is sinus tachycardia at ~105/minute. The rhythm is sinus tachycardia at ~115/minute.
She had a history of hypertension, and was on medication for this — but she was otherwise healthy. The ECG in Figure-1 was obtained from an older woman — who presented with chest pain and palpitations over the previous hour. BP = 140/90 mm Hg in association with the rhythm in Figure-1. How would YOU interpret the rhythm in Figure-1 ?
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. Acute myocardial injury: Is it myocardial infarction, or perhaps myocarditis? If it is MI, is it type 1 or type 2? Is it STEMI or NonSTEMI? Is it acute persistent occlusion?
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
POTENTIAL SIDE EFFECTS : While diuretics can be effective in managing symptoms such as edema and hypertension, possible side effects include electrolyte imbalances, dehydration, and hypotension. This can relieve swelling and shortness of breath caused by fluid buildup in the lungs or other parts of the body.
In addition to sinus tachycardia, the only abnormalities listed by the computer were "low voltage, precordial leads" and "anteroseptal infarct, old.Q He was mildly tachycardic (105-110 bpm) and hypertensive (157/92 mm Hg) on arrival. 4) There is well formed J-point notching. Case 2: What do you think?
Hypertension and diabetes were the two most common risk factors identified. were male, with the average age of 56.313.5 The average time to present to the emergency room after symptom onset was 3.7 The majority of patients (67.9%) have been diagnosed with ST- Elevated Myocardial Infarction and were classified as Killip class I.
The patient stated he had a long history of well-controlled hypertension for which he was compliant with his ACE-inhibitor. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. He was also treated for erectile dysfunction but had not taken any medications recently.
My L IST includes the following: i ) LVH with strain; ii ) Ischemia; iii ) Digoxin use; iv ) HypoKalemia and/or HypoMagnesemia; v ) Tachycardia; and , vi ) Any combination of i-thru-v. Does this patient have hypertension and/or heart failure that has worsened? Often more than one entity is operative as is likely in this case.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content