This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Stroke, Volume 56, Issue Suppl_1 , Page ADP36-ADP36, February 1, 2025. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. Additional randomized and controlled clinical research is deserved.
This comprehensive literature review focuses on acute stroke related to intracranial atherosclerotic stenosis (ICAS), with an emphasis on ICAS-large vessel occlusion. Various risk factors, including hypertension, diabetes, hyperlipidemia, smoking, and advanced age lead to ICAS, which in turn results in stroke through different mechanisms.
IntroductionIdiopathic intracranial hypertension (IIH) is a pathology involving an increase in intracranial pressure leading to symptoms including papilledema, tinnitus, and elevated cerebrospinal fluid opening pressure. Ophthalmology consult revealed bilateral papilledema, upon which an MRI and MRV revealed venous stenosis.
Introduction:Medical therapy and endovascular therapy for intracranial atherosclerotic disease (ICAD) have evolved over the past two decades with improved medical therapy benchmarks, and improved techniques and patient selection for stenting. There were significantly higher incidences in uncontrolled hypertension (28.2%
IntroductionDrug‐eluting stent (DES) use in symptomatic intracranial atherosclerosis disease (ICAD) has been described in the literature using different guiding and distal access catheters. Decision was made to deploy a drug eluting stent into the stenosed M1 segment. The Phenom intermediate catheter was then removed, and the 2.25
Background:Persistent hypotension after carotid artery stenting (CAS) can lead to adverse outcomes, prolong length of stay (LOS), and increase hospital costs. Conclusion:Prior use of RASI for the treatment of hypertension is associated with persistent hypotension after CAS. Persistent hypotension prolonged LOS (P=0.014).Conclusion:Prior
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chest pain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. Here are other very interesting posts: Wellens' syndrome: to stent or not?
Doppler ultrasonography performed a day after the operation showed an increase in systolic blood velocity, with no observed urine output and raising a suspicion of arterial anastomotic stenosis. The transplant renal artery lesion was intervened with a stent.
Background:Vertebrobasilar artery stenosis (VBAS) can cause posterior circulation strokes (PCS). Optimal management is controversial, with options including medical therapy (MT), endovascular stenting (ES), and surgical revascularization (SR). Hypertension (HTN, 85.4%) and diabetes (DM, 18.9%) were prevalent. Mean age was 69.45
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
MRA head demonstrated multifocal arterial stenosis. She was treated with intravenous hydration, permissive hypertension with head of bed in flat position and transferred for further evaluation. MRI brain showed subacute infarcts in left greater than right frontal lobes, corpus collosum and right anterior perforated substance.
Patients with dextrocardia present a diagnostic challenge, particularly in the context of acute coronary syndrome.Case Presentation:A 49-year-old male with a medical history of dextrocardia, hypothyroidism, dyslipidemia and hypertension was referred to a cardiologist by his primary physician due to a 3-week history of unstable angina.
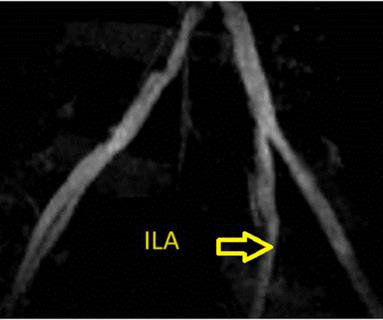
If the pulmonary anatomy is poor, there will be post repair right ventricular hypertension, which is deleterious and has long term seqeulae. Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery. If McGoon’s ratio is below 0.8,
Our case describes a patient with right extracranial internal carotid artery (ICA) thrombus secondary to later‐diagnosed CaW on close follow‐up imaging.MethodsWe report a 55‐year‐old African American man with history of hypertension, type 2 diabetes mellitus and hyperlipidemia presented with acute onset slurred speech and left facial droop (FP).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. The red arrow points to a 90% stenosis in the proximal segment of the LAD. RAO Caudal view: This is the RAO Caudal view.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. The culprit mid LAD lesion was stented. Chest Pain – Benign Early Repol or OMI?
Patient underwent emergent mechanical thrombectomy with ADAPT to TICI3 revascularization with future plan for possible angioplasty and stenting of R vertebral stenosis. CT perfusion was without mismatch. Subsequently admitted to neurocritical care unit and treated with dual antiplatelet therapy.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Two stents were placed with resultant TIMI 3 flow.
A woman in her 40's who was healthy, except for hypertension, was at work when she suddenly complained of neck and shoulder pain and then collapsed. It was stented. It was witnessed, and CPR was performed by trained individuals. Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). If it is MI, is it type 1 or type 2?
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. The patient was found to be hypertensive and treated accordingly. There may even be significant overlap between these factors.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow. Here is his ECG on arrival: What do you think?
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. A mid-LAD culprit lesion was identified and stented.
Marked differences can be seen in the prevalence of coronary artery stenosis at autopsy by age and gender. In 30-39 year old women the rate of coronary stenosis at autopsy was 5/1,545 (0.3%) while 60-69 year old men had a prevalence of 12%, almost 40 times higher. The results of this dataset by age and gender follow.
Recent literature has demonstrated that the Resolute Onyx Zotarolimus‐Eluting stent (RO‐ZES) is a technically safe option with low complication rates. Further prospective multicenter studies are needed to corroborate the findings and compare RO‐ZES directly with other stents. in the RO‐ZES group and 35.6% 8.96, p=0.001).ConclusionThe
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
hypertension no other past history presented with 30 minutes of fluctuating non-radiating heaviness in chest, with diaphoresis and nausea. Here is the angiogram: Very tight stenosis in circumflex, but with TIMI-3 flow, thanks to thrombolytics. This case was sent by an old residency friend, Kirk Lufkin. Case A 61 year old female.
He carries the diagnoses hyperlipidemia, hypertension, and diabetes. First obtuse marginal also had an 80% stenosis and was stented. Here is the cardiology note, paraphrased to make it not identifiable: 50-something seen in cardiology consultation today at the request of Dr. XXXXXX for an NSTEMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content