This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. The conventional machine algorithm interpreted this ECG as STEMI. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chest pain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Past medical history included diabetes and hypertension.
This was sent by a recent ultrasound fellow, asking for my ECG diagnosis. He stated that it is "an acute change from previous" in an elderly smoker with hypertension, syncope, and abdominal pain. However, there are morphologies of Takotsubo that cannot be distinguished from STEMI. Here are some examples: 1.
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chest pain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. It was not a STEMI) 1.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. On medic arrival, she walked out of the house in no distress, but was diaphoretic.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Any indications for cath lab activation?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Smith comment: This patient did not have a bedside ultrasound. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. What should be done?
They recorded a prehospital ECG and diagnosed STEMI and activated the cath lab prehospital. ALL TROPS WERE UNDETECTABLE A formal ultrasound was done: Normal estimated left ventricular ejection fraction at rest. When medics arrived, he denied any chest pain, shortness of breath, or palpitations prior to the syncopal episode.
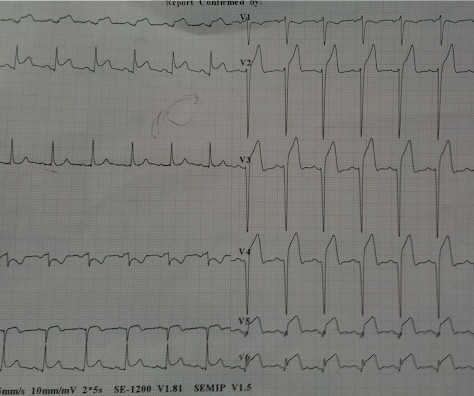
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 Learning Points: 1.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Even the Queen can be wrong.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism. What do you think?
A bedside cardiac ultrasound was normal, with no effusion. Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 Median age was 66.4
A 30-something woman with chest pain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chest pain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. The patient's initial troponin I was 2.0 ng/mL (99% reference level = 0.030 ng/mL. With his ESRD, he does have an elevated baseline troponin at ~0.40
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. And almost all of them could be detected by bedside ultrasound.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chest pain radiating into both arms as well as his back and jaw. Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day.
These ECGs were texted to me by one of our previous ultrasound fellows, Will Smoot An elderly male arrived via EMS for acute substernal chest pain with radiation to left shoulder and arm that awakened him from sleep at 0030. PMHX significant for hypertension and BPH. He took two full strength aspirin prior to EMS arrival.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content