This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! The hypertension alone is the likely etiology of the pulmonary edema. He had no chest pain.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
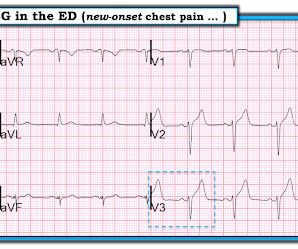
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
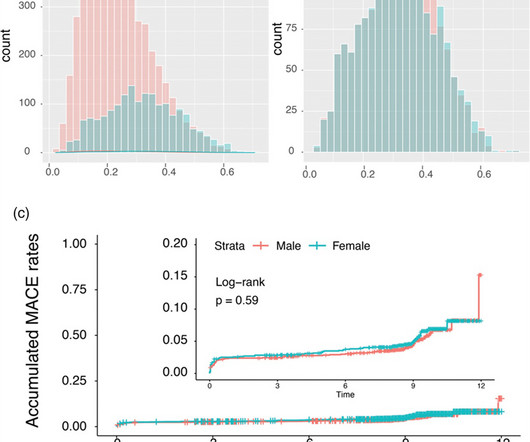
The purpose of this report is to use propensity score matching to determine gender-specific differences in clinical outcomes after percutaneous coronary interventions with polymer-free sirolimus-coated stents. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001).
He learned more about the patient: A 77 year old female with a past medical history of hypertension and hyperlipidemia presented to the ED at around 0520 after waking up at 0400 with 10/10 chest heaviness radiating to both arms. There was a 100% proximal LAD occlusion that was opened and stented. The cath lab was activated.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. This ECG was read as “No STEMI” with no prior available for comparison.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chest pain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. Patient still not having chest pain however this is more concerning for OMI/STEMI. Aspirin given. Am J Cardiol.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below).
The overall prevalence of arterial hypertension was 33.2%, hyperlipidemia, 26.9%, smoking, 17.8%, and diabetes, 3.9%. with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5% and 1.3%, respectively.
Her vitals signs were remarkable for marked hypertension. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." The criteria of Armstrong et al. References 1.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Here is the angiogram after stent placement. Immediate versus delayed invasive intervention for non-stemi patients. Marinkovic, J.,
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chest pain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Even the Queen can be wrong.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
She is somewhat hypertensive, but her vital signs are otherwise normal. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. This case is tough.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Time zero: What do you think?
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. mm STE in one lead.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
Vital signs were noted to be unremarkable with respect to any hypo-hypertensive crisis, hypoxia, etc. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Breath sounds were clear in all lung fields.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3 It was stented.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. So the RCA was stented.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. Am J Emerg Med. 2014;32:e5–e8.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high).
He had a history of hypertension, but no history of heart problems. Computer interpretation: SINUS RHYTHM NON-DIAGNOSTIC ANTEROLATERAL ST ELEVATION BORDERLINE ECG The overreading cardiologist confirmed the computer interpretation (did not diagnose OMI or STEMI). Since the threshold for "STEMI" is 2.0 LAD occlusion.
A woman in her 40's who was healthy, except for hypertension, was at work when she suddenly complained of neck and shoulder pain and then collapsed. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. It was stented. It was witnessed, and CPR was performed by trained individuals.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
He was hypertensive and tachycardic, with mildly increased work of breathing. The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Is this inferor STEMI? What is the Diagnosis?
This is by Magnus Nossen, from Norway The patient is a 70 something male with a hx of hypertension and tobacco use disorder. The culprit lesion was opened and stented. He is otherwise healthy. The patient contacted EMS after a few hours of chest pain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder.
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. The patient was found to be hypertensive and treated accordingly. STEMI was activated and the patient went to Cath on arrival.
The patient stated he had a long history of well-controlled hypertension for which he was compliant with his ACE-inhibitor. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. He was also treated for erectile dysfunction but had not taken any medications recently.
He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia. He was taken to the cath lab where he was found to have acute total occlusion of his saphenous vein graft to his RCA, which was stented. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms.
It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. Further diagnostic confusion may have resulted from the greater prevalence of hypertension and likely attendant hypertensive heart disease and uninterpretable ST depression in the dialysis cohort.” Herzog et al.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. Written by Emre Aslanger.
hypertension no other past history presented with 30 minutes of fluctuating non-radiating heaviness in chest, with diaphoresis and nausea. But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. This case was sent by an old residency friend, Kirk Lufkin. Case A 61 year old female.
Written by Magnus Nossen The ECG below was obtained from 50-something male with a history of hypertension and tobacco use. This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. At cath there was a 100% proximal LAD occlusion, which was opened and stented. How will you manage this patient?
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chest pain at 2343. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent").
He has a history of hypertension an d tobacco use. The CAG showed a 99% thrombotic lesion of the proximal RCA, which was stented. Written by Magnus Nossen The below ECG was obtained from a 65 year old man with ongoing chest pain. He is otherwise healthy. There is no prior ECG for comparison. What do you think?
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". He carries the diagnoses hyperlipidemia, hypertension, and diabetes. First obtuse marginal also had an 80% stenosis and was stented. Pt received 324 ASA and 2 sprays of nitro with improvement. Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content